

Glaucoma and refractive surgery: A comprehensive review
- PMID: 39185827
- PMCID: PMC11552800
- DOI: 10.4103/IJO.IJO_3236_23
Glaucoma and refractive surgery: A comprehensive review
Abstract
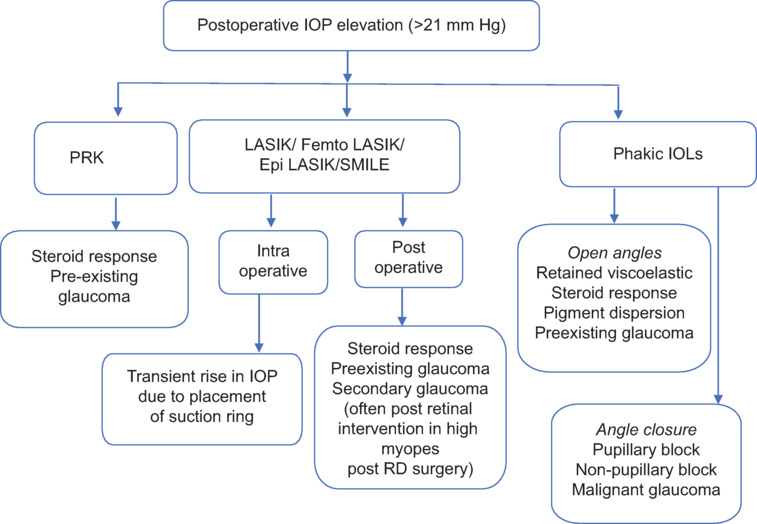
The global surge in refractive surgeries, particularly among myopic individuals, has elicited concerns regarding potential inaccuracies in the measurement of intraocular pressure (IOP) post surgery, primarily associated with central corneal thinning. The incidence of elevated IOP after intraocular refractive surgeries is higher than expected and is multifactorial. Myopic eyes have a higher susceptibility to both primary and secondary glaucoma. Consequently, meticulous preoperative screening for glaucoma is imperative, coupled with systematic postoperative follow-up and evaluation. This comprehensive review analyses the etiology, mechanisms, and therapeutic strategies for managing elevated IOP following refractive surgery. We propose an algorithm to summarize the causative factors of elevated IOP and formulate effective interventions in these instances.
Copyright © 2024 Copyright: © 2024 Indian Journal of Ophthalmology.
Conflict of interest statement
There are no conflicts of interest.
Figures









References
-
- Kersey JP, Broadway DC. Corticosteroid-induced glaucoma: A review of the literature. Eye (Lond) 2006;20:407–16. - PubMed
-
- Mitchell P, Hourihan F, Sandbach J, Wang JJ. The relationship between glaucoma and myopia: The Blue Mountains eye study. Ophthalmology. 1999;106:2010–5. - PubMed
-
- Xu L, Wang Y, Wang S, Wang Y, Jonas JB. High myopia and glaucoma susceptibility the Beijing Eye Study. Ophthalmology. 2007;114:216–20. - PubMed
-
- Perkins ES, Phelps CD. Open angle glaucoma, ocular hypertension, low-tension glaucoma, and refraction. Arch Ophthalmol. 1982;100:1464–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
