

Intermittent Energy Restriction for Adolescents With Obesity: The Fast Track to Health Randomized Clinical Trial
- PMID: 39186288
- PMCID: PMC11348084
- DOI: 10.1001/jamapediatrics.2024.2869
Intermittent Energy Restriction for Adolescents With Obesity: The Fast Track to Health Randomized Clinical Trial
Abstract
Importance: Adolescent obesity requires effective and accessible treatment. Intensive dietary interventions have the potential to be used as adjunctive therapy for behavioral weight management.
Objective: To examine the effectiveness of 2 diet therapies, delivered as part of an intensive behavioral weight management intervention, in adolescents with metabolic complications associated with obesity.
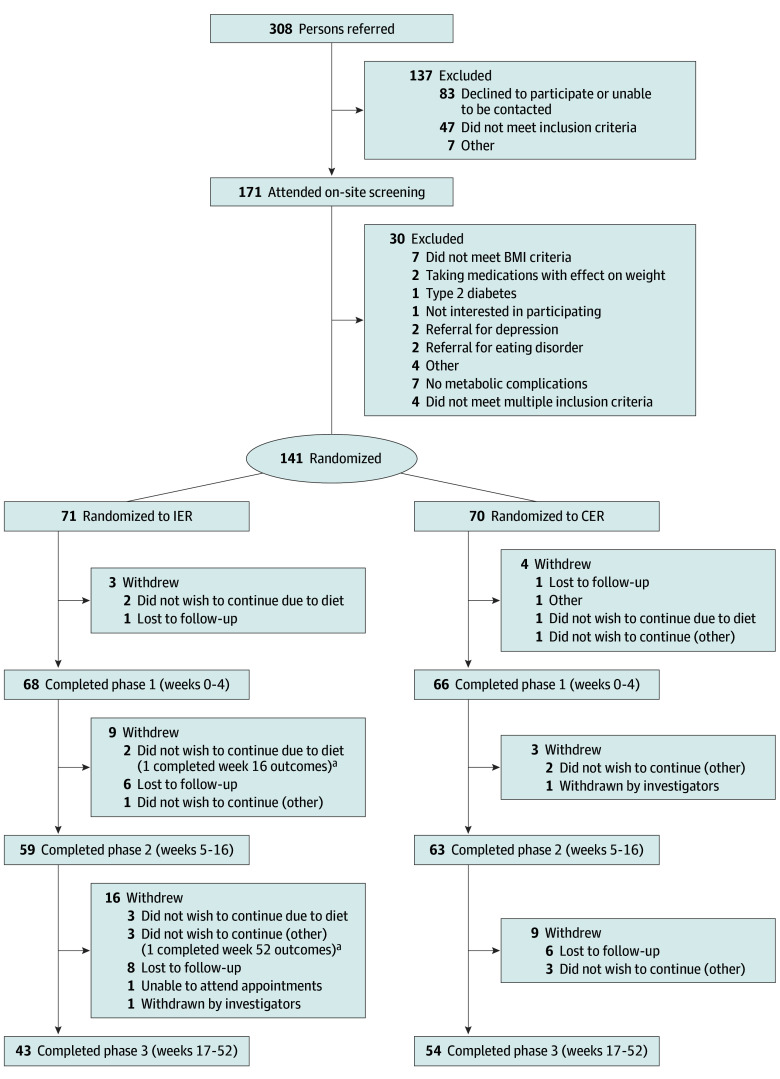
Design, setting, and participants: This multisite, 52-week randomized clinical trial was conducted from January 31, 2018, to March 31, 2023, at 2 tertiary pediatric centers in Australia. Adolescents (aged 13-17 years) with obesity and 1 or more associated complications were included.
Interventions: Intensive behavioral interventions, delivered by a multidisciplinary team, comparing intermittent energy restriction (IER) or continuous energy restriction (CER), with 3 phases: very low-energy diet (weeks 0-4), intensive intervention (weeks 5-16), and continued intervention and/or maintenance (weeks 17-52).
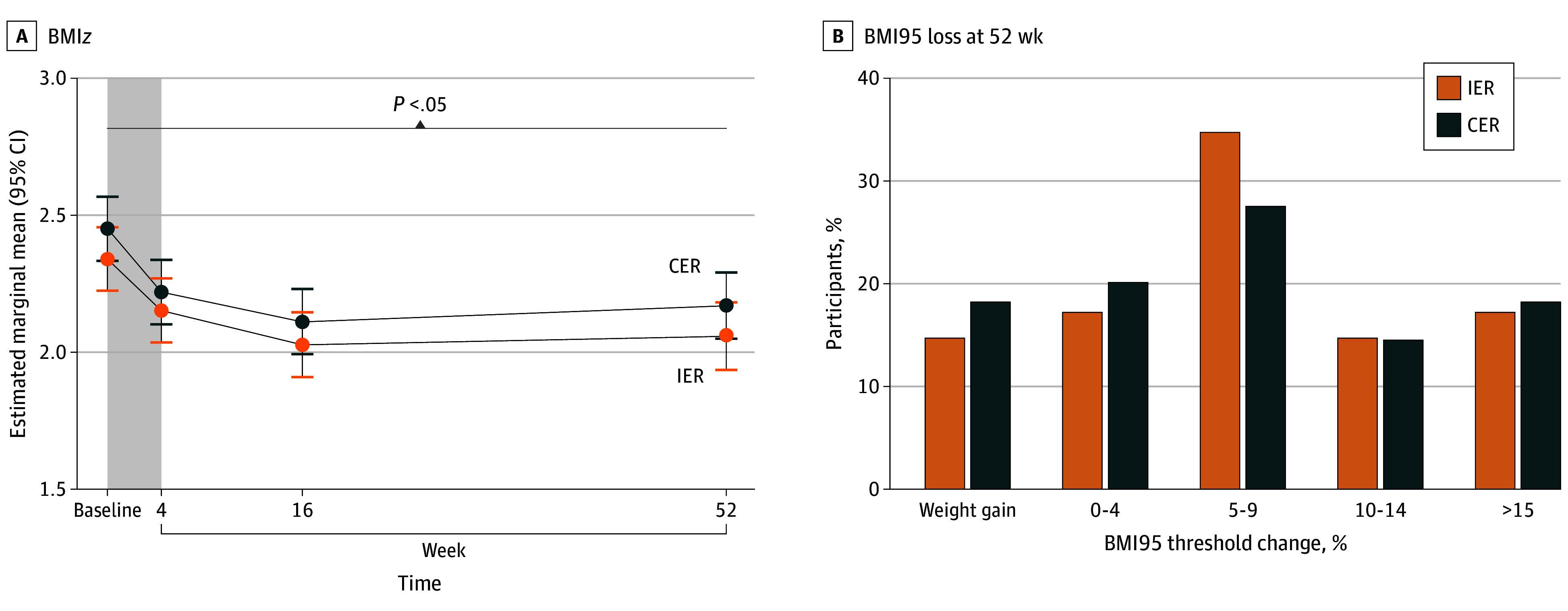
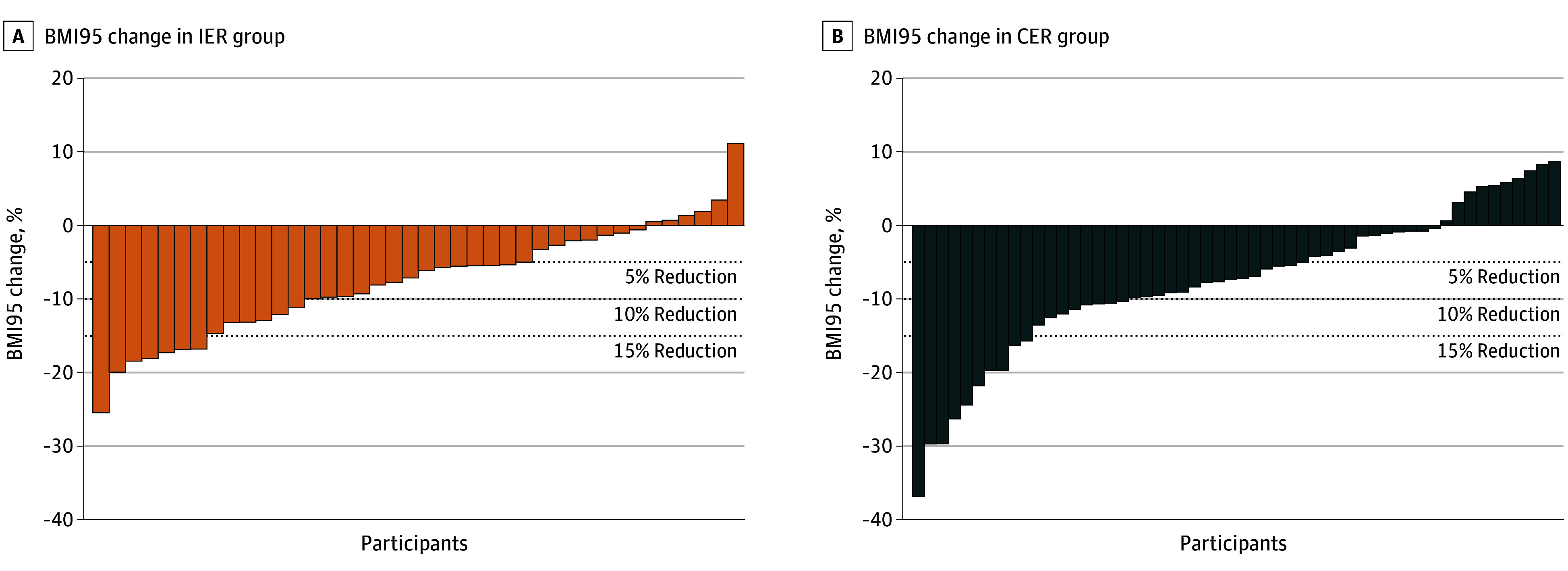
Main outcomes and measures: The primary outcome was body mass index (BMI) z score at 52 weeks in the IER vs CER group. Anthropometry, body composition, and cardiometabolic health were assessed at baseline and 52 weeks. The BMI z score and percentiles were determined using Centers for Disease Control and Prevention growth charts. Insulin resistance, dyslipidemia, and elevated hepatic function were assessed.
Results: A total of 141 adolescents (median [IQR] age, 14.8 [12.9-17.9] years; 71 male [50.4%]) were enrolled, 71 in the IER group and 70 in the CER group, and 97 (68.8%) completed the intervention, 43 in the IER group and 54 in the CER group. At week 52, both groups had reduced BMI z scores (estimated marginal mean change, -0.28 [95% CI, -0.37 to -0.20] for IER and -0.28 [95% CI, -0.36 to -0.20] for CER) and reduced BMI expressed as a percentage of the 95th percentile (estimated marginal mean change, -9.56 [95% CI, -12.36 to -6.83] for IER and -9.23 [95% CI, -11.82 to -6.64] for CER). No differences were found in body composition or cardiometabolic outcomes between the groups. Both groups had a reduction in the occurrence of insulin resistance (from 52 of 68 [76.5%] to 32 of 56 [57.1%] in the IER group and from 59 of 68 [86.8%] to 31 of 60 [57.1%] in the CER group) at week 16; however, at week 52, this effect was observed in the CER group only (from 59 of 68 [86.7%] to 30 of 49 [61.2%]). The occurrence of dyslipidemia was unchanged between baseline and week 52 (60 of 137 [42.6%] and 37 of 87 [42.5%], respectively), with a small improvement in occurrence of impaired hepatic function tests (37 of 139 [27.0%] and 15 of 87 [17.2%], respectively). No differences were found in dyslipidemia or hepatic function between groups.
Conclusions and relevance: These findings suggest that for adolescents with obesity-associated complications, IER can be incorporated into a behavioral weight management program, providing an option in addition to CER and offering participants more choice.
Trial registration: http://anzctr.org.au Identifier: ACTRN12617001630303.
Conflict of interest statement
Figures
References
-
- Lobstein T, Brinsden H. Atlas of Childhood Obesity. World Obesity Federation; 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
