

Clinically important changes and adverse events with centre-based or home-based pulmonary rehabilitation in chronic respiratory disease: A systematic review and meta-analysis
- PMID: 39187265
- PMCID: PMC11348370
- DOI: 10.1177/14799731241277808
Clinically important changes and adverse events with centre-based or home-based pulmonary rehabilitation in chronic respiratory disease: A systematic review and meta-analysis
Abstract
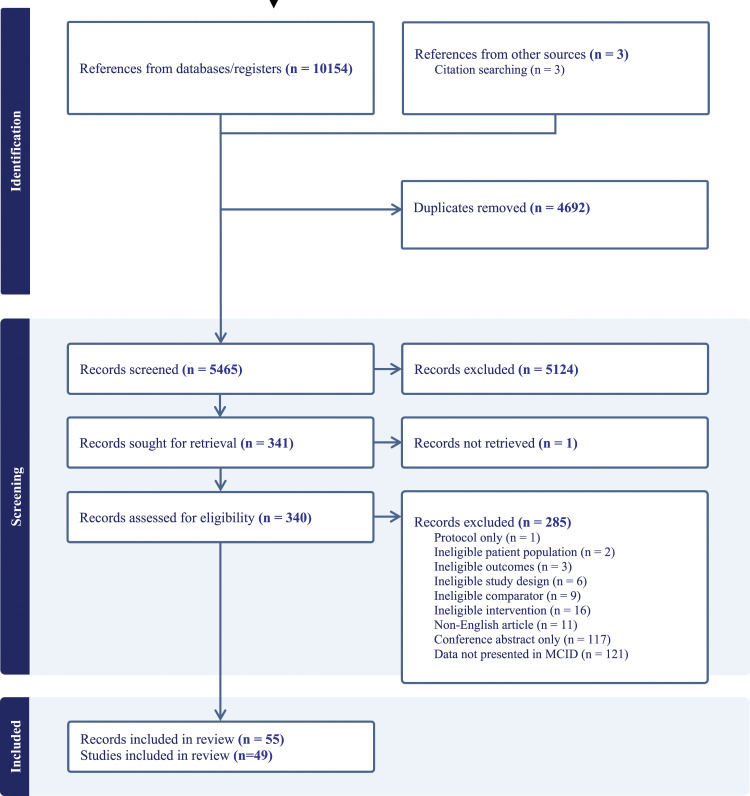
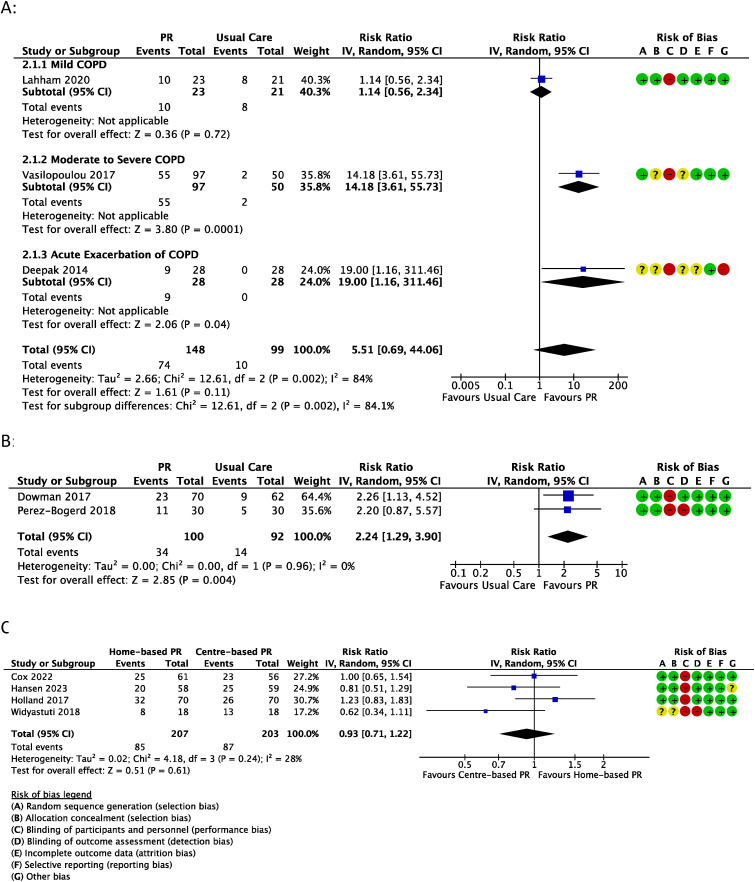
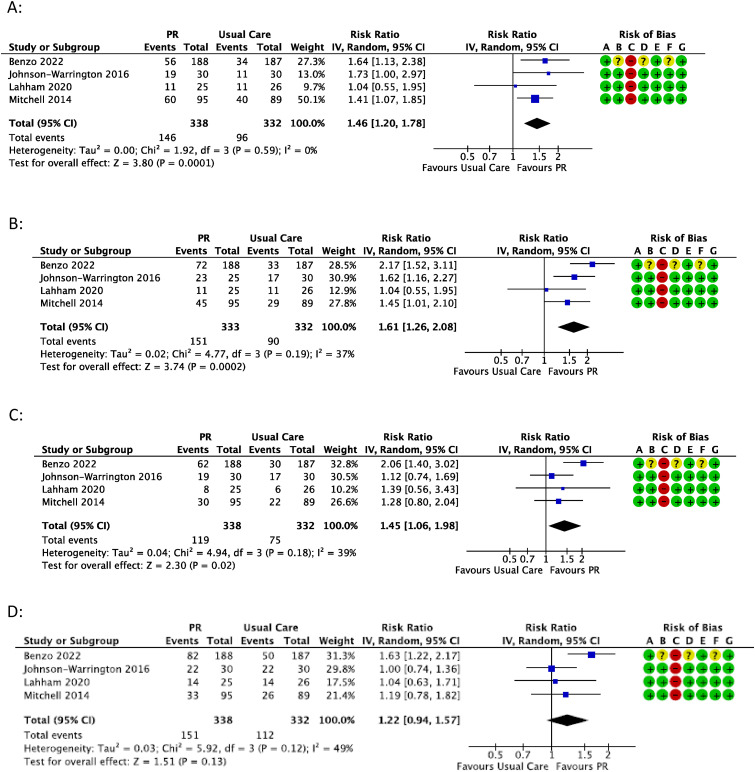
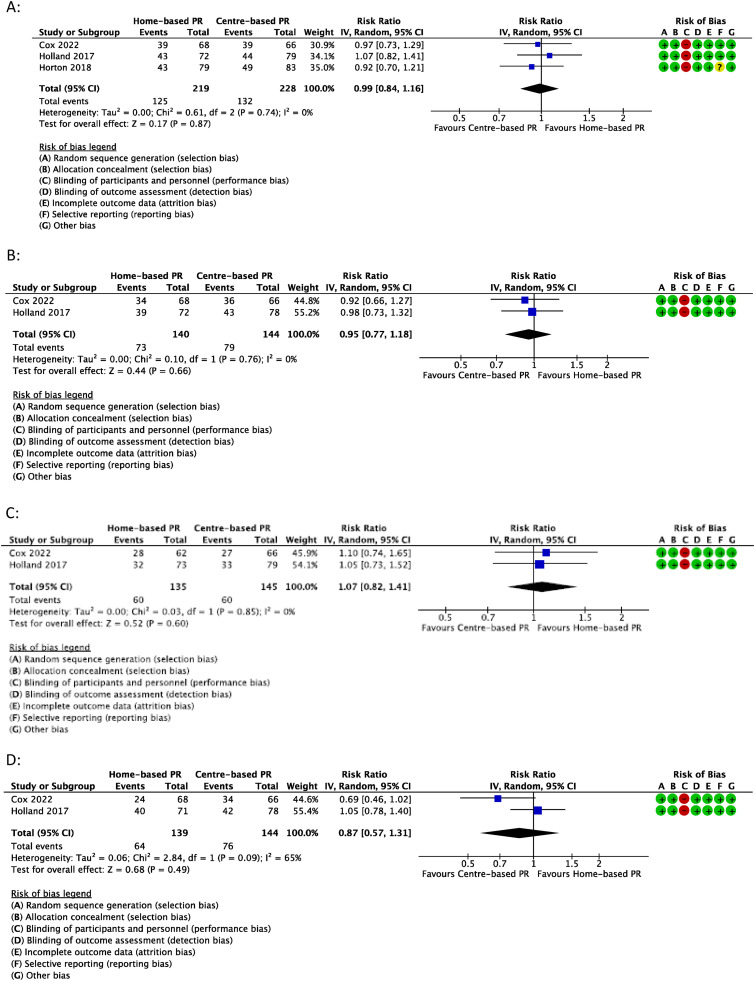
Objectives: To determine the proportion of people who achieve minimal clinically important differences (MCID) with centre-based or home-based pulmonary rehabilitation and to synthesise data on adverse events.Methods: Cochrane reviews and electronic databases were searched to identify randomised trials comparing centre-based to home-based pulmonary rehabilitation, or either model to usual care, in people with chronic respiratory disease. Primary outcomes were the proportion of participants achieving MCIDs in exercise capacity and disease-specific quality of life. Secondary outcomes were symptoms and adverse events. Cochrane Risk of Bias 1.0 and GRADE were used to assess the risk of bias and certainty of evidence respectively.Results: Forty-nine trials were eligible. Compared to usual care, a higher proportion of pulmonary rehabilitation participants achieved the MCID for exercise capacity (6MWT: 47% vs 20%, p = 0.11), dyspnoea (43% vs 29%, p = 0.0001), fatigue (48% vs 27%, p = 0.0002) and emotional function (37% vs 25%, p = 0.02), with all of these between group differences statistically significant except for exercise capacity. There were no differences between centre-based and home-based pulmonary rehabilitation in the proportion of participants who achieved MCIDs (34%- 58% across studies). Ninety percent of trials reported no adverse events. Certainty of evidence was low-to- moderate with all outcomes except for CRQ-mastery (centre-based vs home-based pulmonary rehabilitation, or pulmonary rehabilitation vs usual care in COPD), ESWT (pulmonary rehabilitation vs usual care in COPD) and 6MWT (pulmonary rehabilitation vs usual care in bronchiectasis) where evidence was very uncertain.Discussion: Clinically meaningful outcomes are achieved by similar proportions of participants in centre-based and home-based pulmonary rehabilitation, with few adverse events. Reporting of trial outcomes according to MCIDs is necessary for informed decision making regarding pulmonary rehabilitation models.
Keywords: Chronic obstructive pulmonary disease; bronchiectasis; exercise training; interstitial lung disease; rehabilitation.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- GBD 2017 DALYs and HALE Collaborators . Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet 2018; 392(10159): 1859–1922. - PMC - PubMed
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) . Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2023. https://goldcopd.org/2023-gold-report-2/(Accessed 5 January 2023).
-
- Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J 2017; 50(3): 1700629. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
