

U-shaped correlation of lymphocyte count with all-cause hospital mortality in sepsis and septic shock patients: a MIMIC-IV and eICU-CRD database study
- PMID: 39187746
- PMCID: PMC11346189
- DOI: 10.1186/s12245-024-00682-6
U-shaped correlation of lymphocyte count with all-cause hospital mortality in sepsis and septic shock patients: a MIMIC-IV and eICU-CRD database study
Abstract
Background: In sepsis, the relationship between lymphocyte counts and patient outcomes is complex. Lymphocytopenia and lymphocytosis significantly influence survival, illustrating the dual functionality of lymphocytes in responding to infections. This study investigates this complex interaction, focusing on how variations in lymphocyte counts correlate with all-cause hospital mortality among sepsis patients.
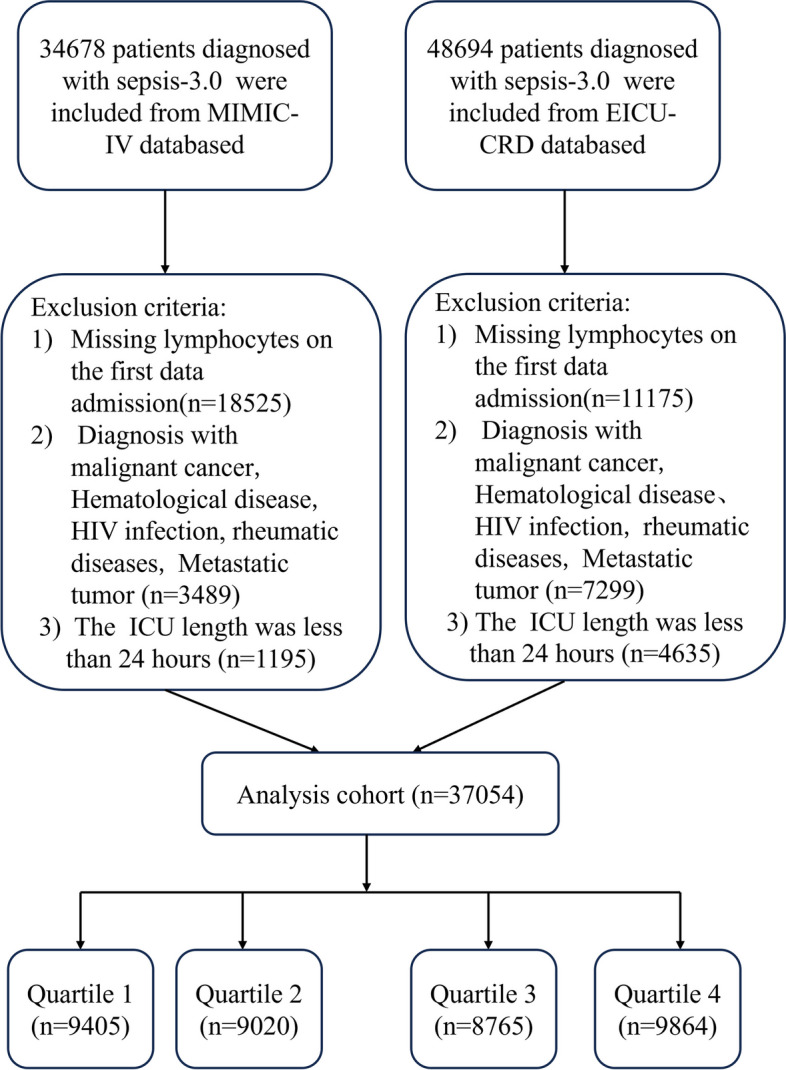
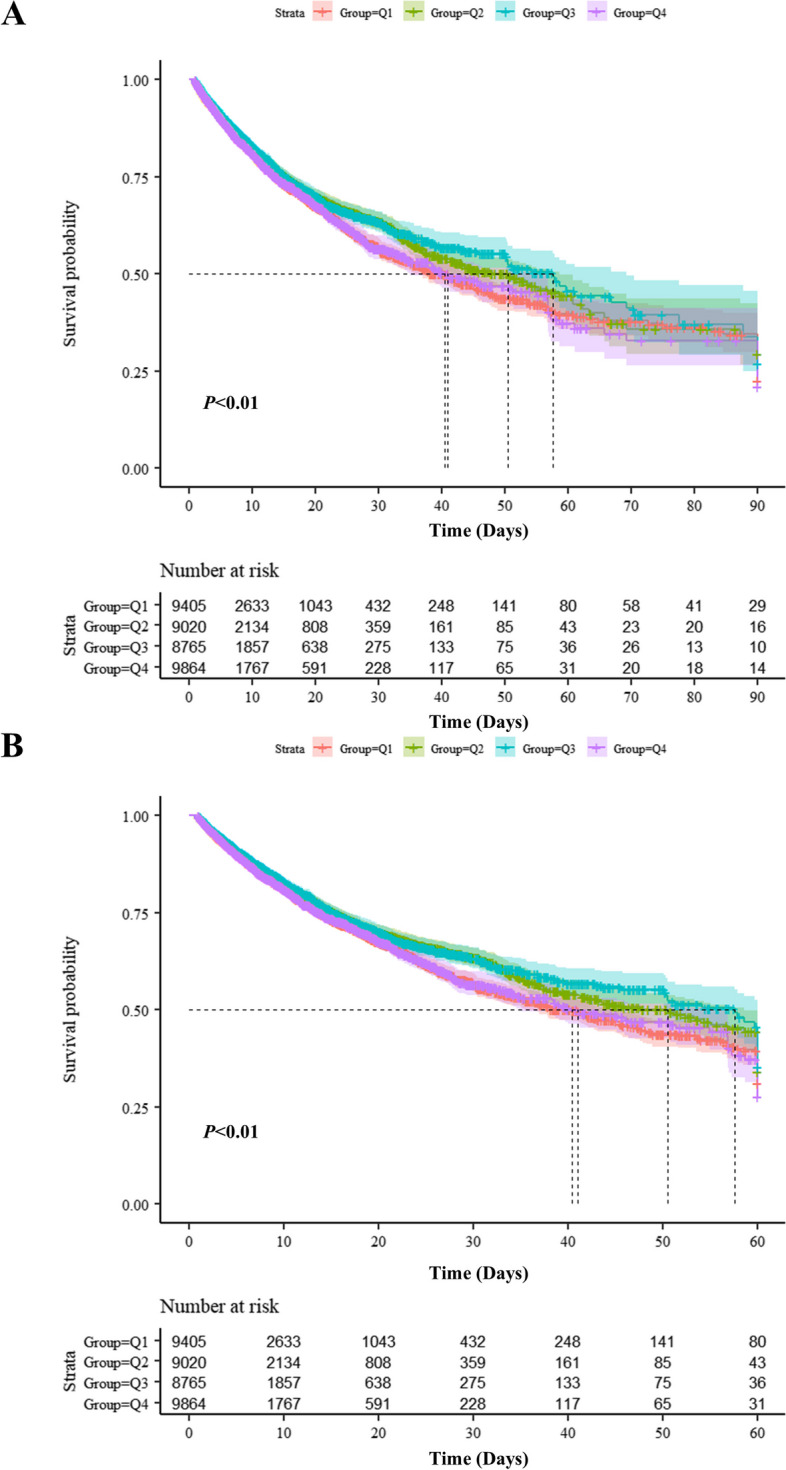
Methods: This retrospective cohort study analyzed data from two extensive critical care databases: the Medical Information Mart for Intensive Care IV 2.0 (MIMIC-IV 2.0) from Beth Israel Deaconess Medical Center, Boston, Massachusetts, and the eICU Collaborative Research Database (eICU-CRD), which was Multi-center database from over 200 hospitals across the United States conducted by Philips eICU Research Institute. We included adult patients aged 18 years and older who met the Sepsis-3 criteria, characterized by documented or suspected infection and a Sequential Organ Failure Assessment (SOFA) score of 2 or higher. Sepsis patients were categorized into quartiles based on lymphocyte counts. The primary outcome was all-cause mortality in the hospital, with 90 and 60-day all-cause mortality as the secondary outcomes. Univariable and multivariable Cox proportional hazard regressions were utilized to assess lymphocyte counts' impact on hospital mortality. An adjusted restricted cubic spline (RCS) analysis was performed to elucidate this relationship further. Subgroup analyses were also conducted to explore the association across various comorbidity groups among sepsis and septic shock patients.
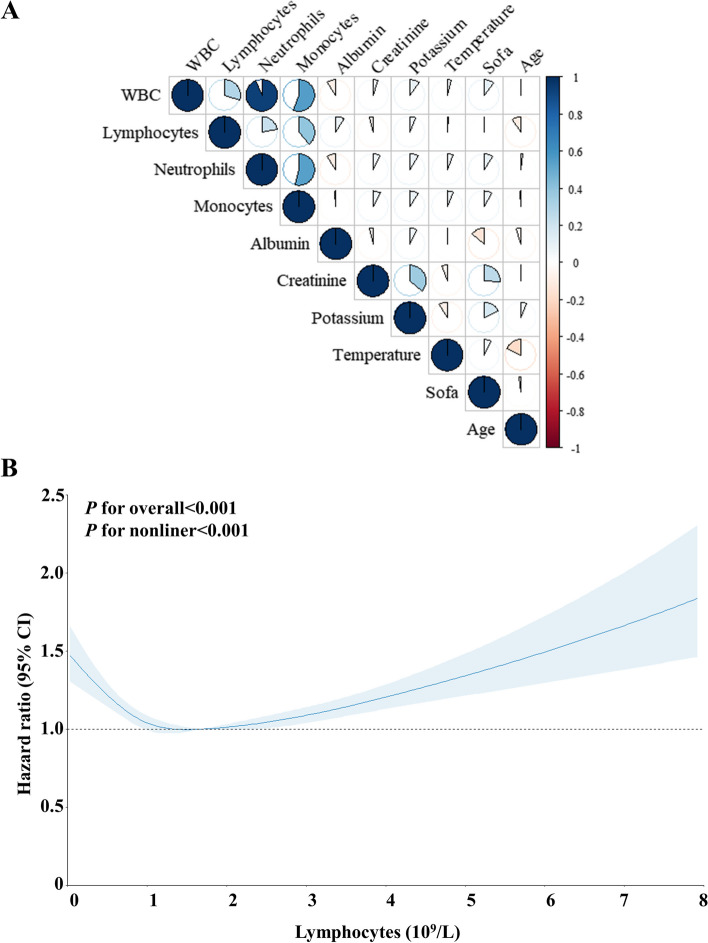
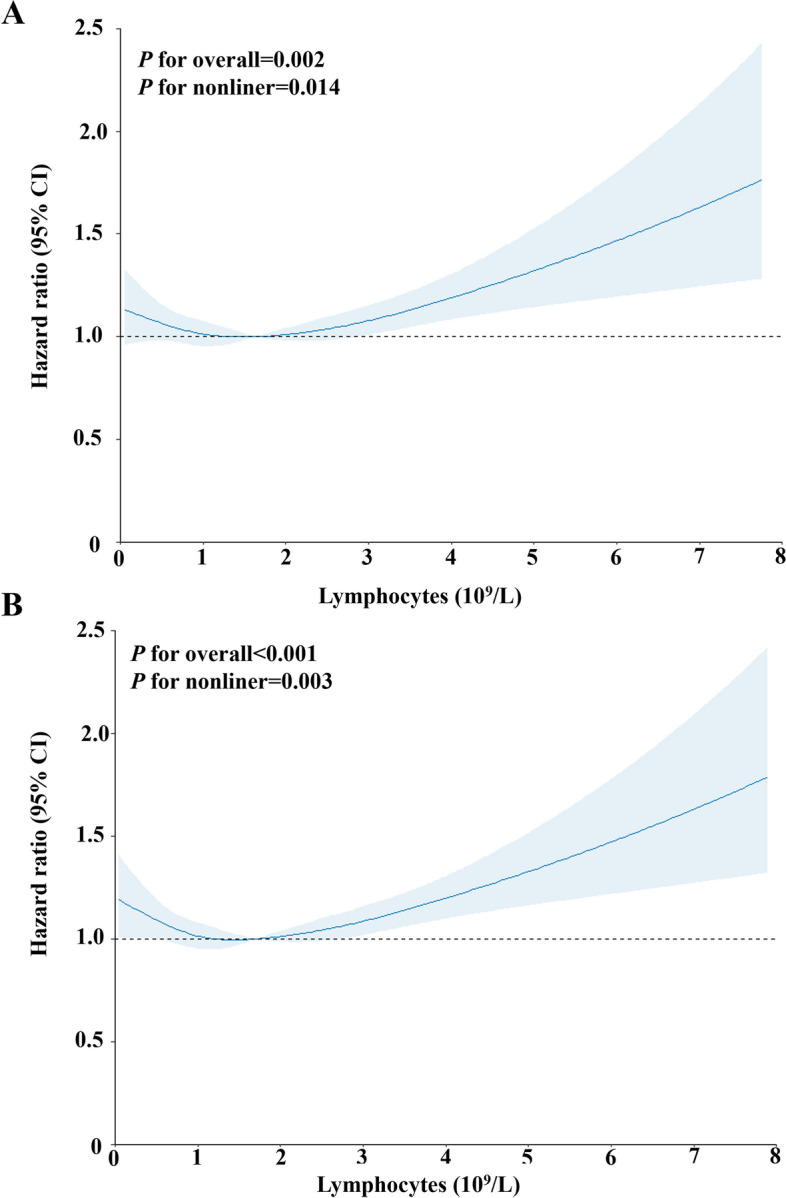
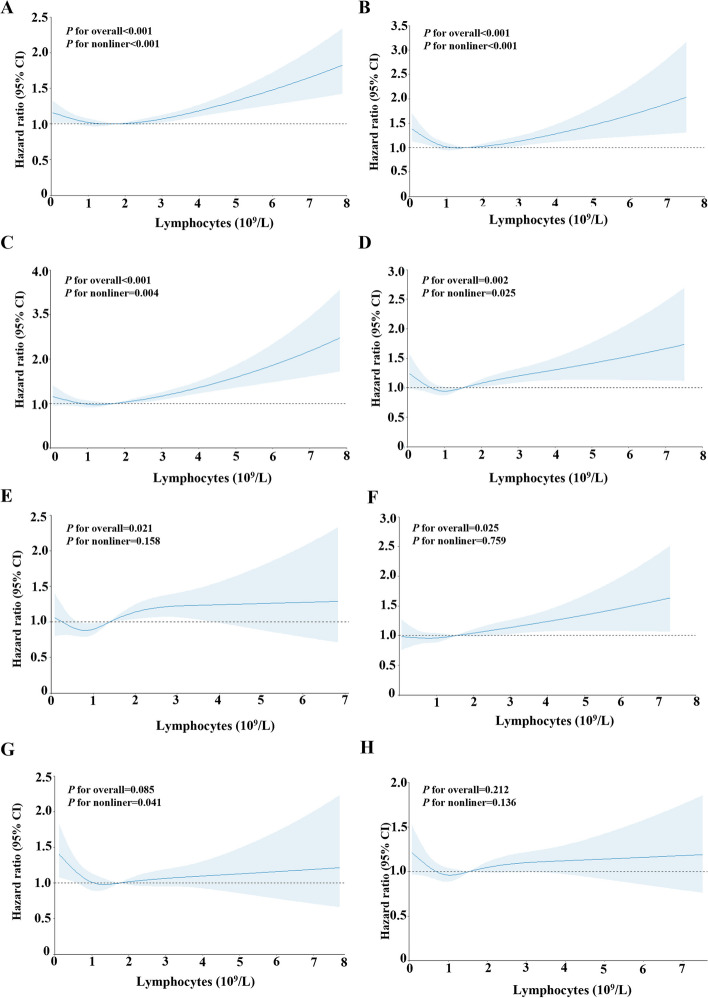
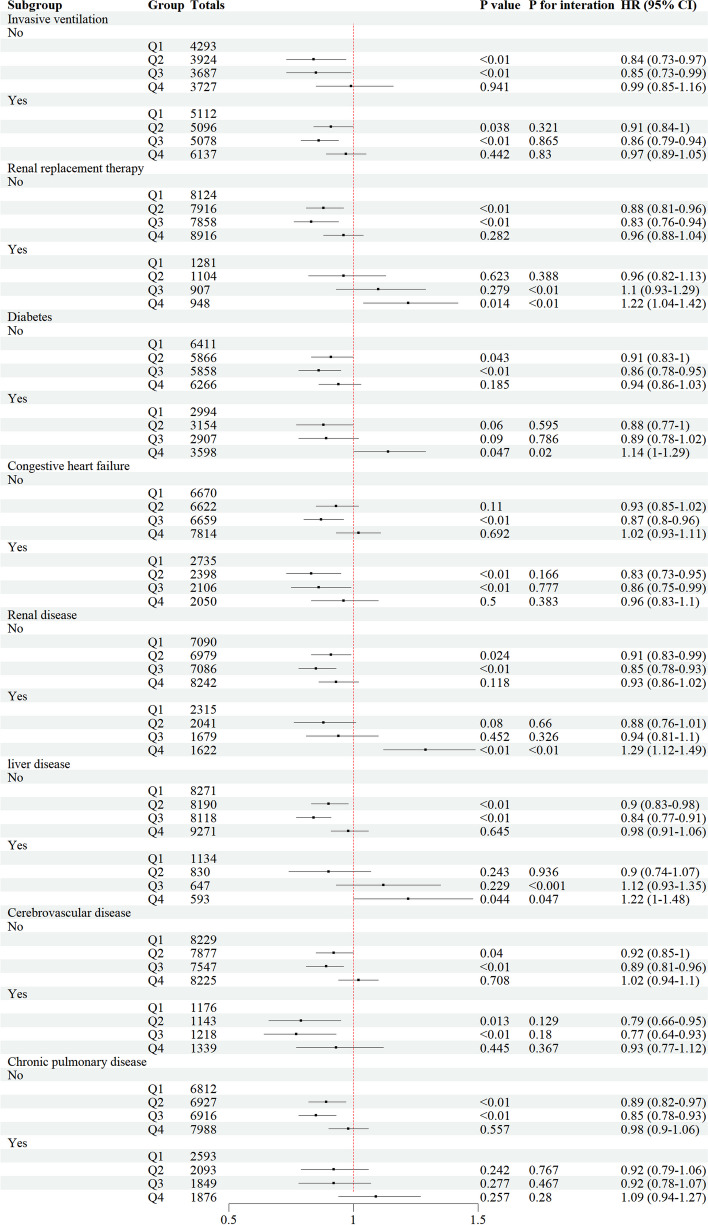
Results: Our study included 37,054 patients, with an observed in-hospital mortality rate of 16.6%. Univariable and multivariable Cox proportional hazard regression models showed that lymphocyte counts were independently associated with in-hospital mortality (HR = 1.04, P < 0.01; HR = 1.06, P < 0.01). RCS regression analysis revealed a U-shaped relationship between lymphocyte levels and hospital mortality risk in sepsis and septic shock patients (P for overall < 0.001, P for nonliner < 0.01; P for overall = 0.002, P for nonliner = 0.014). Subgroup analyses revealed that elevated lymphocyte counts correlated with increased hospital mortality among sepsis patients with liver disease and requiring renal replacement therapy (P for overall = 0.021, P for nonliner = 0.158; P for overall = 0.025, P for nonliner = 0.759). These findings suggest that lymphocytes may have enhanced prognostic value in specific subsets of critically ill sepsis patients.
Conclusion: Our findings demonstrate that lymphocyte counts are a significant independent predictor of hospital mortality in sepsis and septic shock patients. We observed a U-shaped association between lymphocyte levels and mortality risk, indicating that high and low counts are linked to increased mortality. This result highlights the complex role of lymphocytes in sepsis outcomes and suggests the need for further investigation into the underlying mechanisms and potential therapeutic approaches. Integrating lymphocyte count assessment into risk stratification algorithms and clinical decision support tools could enhance the early identification of high-risk sepsis patients.
Keywords: Intensive care unit; Lymphocyte counts; Prediction; Restricted cubic spline; Sepsis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
