

The efficacy of cuff-shaving combined with negative pressure wound therapy in refractory exit-site and tunnel infections: a single center experience
- PMID: 39187762
- PMCID: PMC11346171
- DOI: 10.1186/s12882-024-03714-8
The efficacy of cuff-shaving combined with negative pressure wound therapy in refractory exit-site and tunnel infections: a single center experience
Abstract
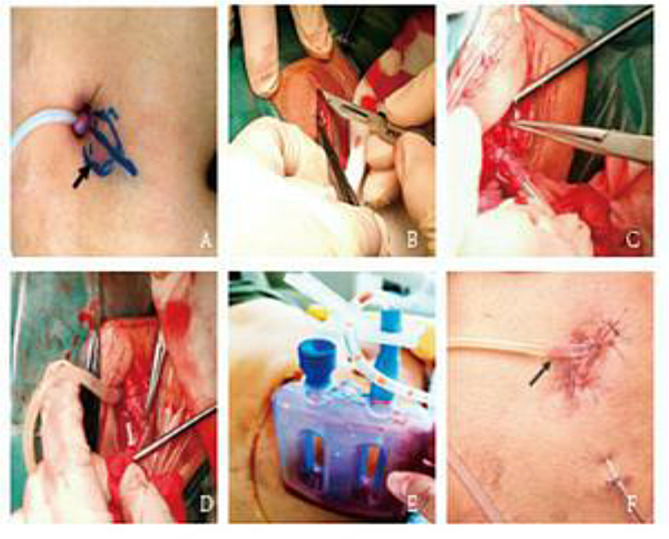
Background: Refractory exit-site infections (ESIs) and tunnel infections (TIs) are challenging complications for patients undergoing peritoneal dialysis (PD). This study compared the outcomes of surgical intervention, notably the cuff-shaving (CS) procedure coupled with negative-pressure wound therapy (NPWT), and conservative management strategies for patients with refractory ESI and TI.
Methods: We retrospectively reviewed patients who underwent PD at our center, focusing on the incidence and management of ESI and TI. We evaluated and compared treatment outcomes, including ESI scores, frequency of ESI and/or TI, identification of causative microorganisms, and duration of catheter survival or time until removal.
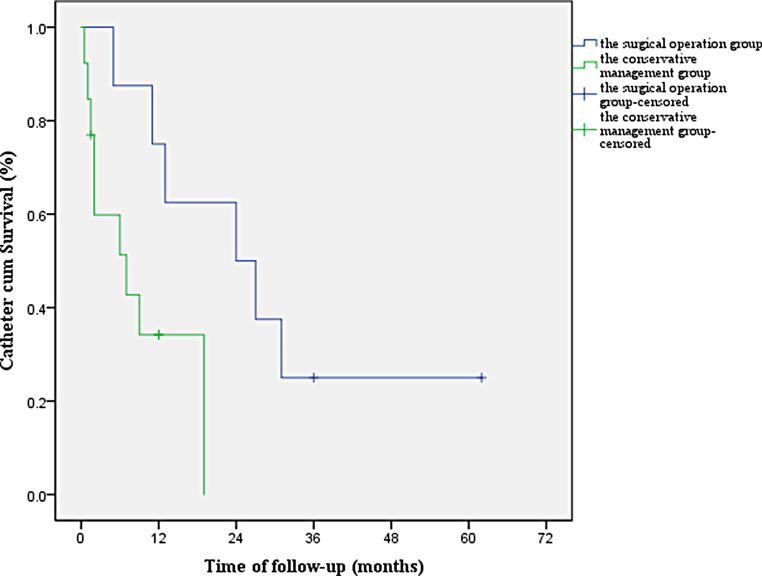
Results: We identified 97 episodes of catheter-related ESI and/or TI across 71 patients with an incidence rate of 0.15 episodes per patient-year. Of the 23 patients with refractory ESI and/or TI, surgical intervention was performed in 8, while 15 chose conservative management. In the one-month follow-up, patients who underwent CS combined with NPWT showed no complications such as leakage, and their local symptoms resolved completely. The mean PD catheter survival time was significantly longer in the surgical group (29.38 ± 7.25 months) than in the conservative group (7.86 ± 2.13 months). Surgical intervention demonstrated a significantly higher therapeutic efficacy and extended catheter survival.
Conclusions: The combination of CS and NPWT as a surgical approach is crucial for eradicating infectious foci and significantly improving the longevity of PD catheter function. This integrated surgical strategy offers a promising solution for the management of refractory ESI and TI in patients undergoing PD.
Keywords: Negative pressure wound therapy; Peritoneal dialysis catheter; Refractory exit-site infection; Superficial cuff-shaving; Tunnel infection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare no conflicts of interest.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
