

The Gradual Correction of Rigid Pes Cavus Using Midfoot Osteotomy Combined with Ilizarov Methods
- PMID: 39187990
- PMCID: PMC11572576
- DOI: 10.1111/os.14206
The Gradual Correction of Rigid Pes Cavus Using Midfoot Osteotomy Combined with Ilizarov Methods
Abstract
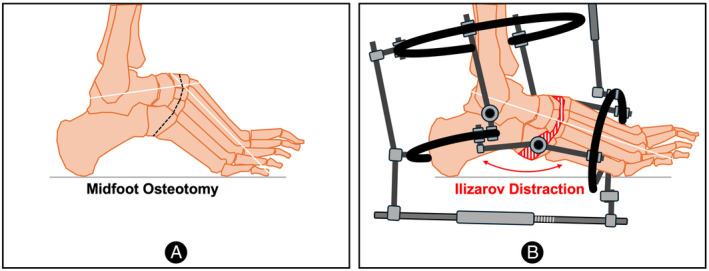
Objective: Midfoot osteotomy combined with Ilizarov methods of correction is a rarely reported treatment that is particularly well-suited for severe rigid pes cavus. The study aimed to assess the radiological and clinical results of patients who had been treated for rigid pes cavus using this method.
Methods: The study retrospectively analyzed the clinical and radiological data of 15 pes cavus in 12 patients who were corrected by midfoot osteotomy with Ilizarov external frame in our department from March 2020 to September 2022. Radiologic outcomes were measured using the Meary angle (MA), talus-first metatarsal angle (TM1A), calcaneal varus angle (CVA) and foot length with weight-bearing radiographs. Functional assessments were evaluated in terms of pain, function, and quality of life by using the visual analogue scale (VAS), the American Orthopedic Foot and Ankle Society hindfoot scale score (AOFAS), and 36-item Short Form Health Survey (SF-36). Additionally, the postoperative satisfaction of patients was investigated by a questionnaire. The clinical and radiological results were evaluated by a paired t-test.
Results: All patients received plantigrade feet and pain relief. The mean follow-up was 33.1 ± 5.0 months (range from 25 to 41 months). The etiology included poliomyelitis (4), idiopathic (3), trauma (2), spina bifida (2) and tethered cord syndrome (1). The duration of gradual correction was 30.4 ± 10.6 days, and the external fixation time was 116.3 ± 33.3 days. The bony union rate was 100%. The VAS, AOFAS, and SF-36 scores significantly improved (p < 0.05). The MA, TM1A, and CVA were close to or reached the normal range postoperative (p < 0.01). The length of each foot was well preserved, which was increased more than 0.8 cm than preoperative. No major complications were reported except two cases of mildly hindfoot varus deformity. The results of the questionnaire showed that patients' satisfaction was 92% (11/12).
Conclusion: Midfoot osteotomy combined with Ilizarov external frame proved to be a reasonable procedure with satisfying mid-term results for the gradual correction of rigid pes cavus.
Keywords: Ilizarov external frame; midfoot osteotomy; pes cavus; tendon transfer.
© 2024 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that they have no conflicts of interest. Ethical approval for all procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or national research committee, and with the 1964 Helsinki Declaration, and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Akoh CC, Phisitkul P. Clinical examination and radiographic assessment of the Cavus foot. Foot Ankle Clin. 2019;24:183–193. - PubMed
-
- Bai L‐B, Wang Z‐J, Wang Z‐T. Telescopic rod technique to reverse anterior subluxation of the talus during the correction of equinocavovarus deformity with the Ilizarov fixator. J Orthop Transl. 2020;25:43–46.
-
- de la Huerta F. Correction of the neglected clubfoot by the Ilizarov method. Clin Orthop Relat Res. 1994;301:89–93. - PubMed
MeSH terms
Grants and funding
- XZ202201ZR0033G/Natural Science Foundation of Tibet Autonomous Region
- XZ202201ZY0038G/Natural Science Foundation of Tibet Autonomous Region
- 2024HXBH076/the full-time postdoctoral research and development fund of West China Hospital of Sichuan University
- 22HXFH015/1·3·5 project for disciplines of excellence-Clinical Research Incubation Project, West China Hospital, Sichuan University
- 2023YFS0014/Natural Science Foundation of Sichuan Province
LinkOut - more resources
Full Text Sources
