

Endoscopic ultrasound-guided hepaticogastrostomy and endoscopic retrograde cholangiopancreatography-guided biliary drainage for distal malignant biliary obstruction due to pancreatic cancer with asymptomatic duodenal invasion: a retrospective, single-center study in Japan
- PMID: 39188118
- PMCID: PMC11837547
- DOI: 10.5946/ce.2024.031
Endoscopic ultrasound-guided hepaticogastrostomy and endoscopic retrograde cholangiopancreatography-guided biliary drainage for distal malignant biliary obstruction due to pancreatic cancer with asymptomatic duodenal invasion: a retrospective, single-center study in Japan
Abstract
Background/aims: Duodenal invasion (DI) is a risk factor for early recurrent biliary obstruction (RBO) in endoscopic retrograde cholangiopancreatography-guided biliary drainage (ERCP-BD). Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) may reduce early RBO in cases of asymptomatic DI, even when ERCP is possible.
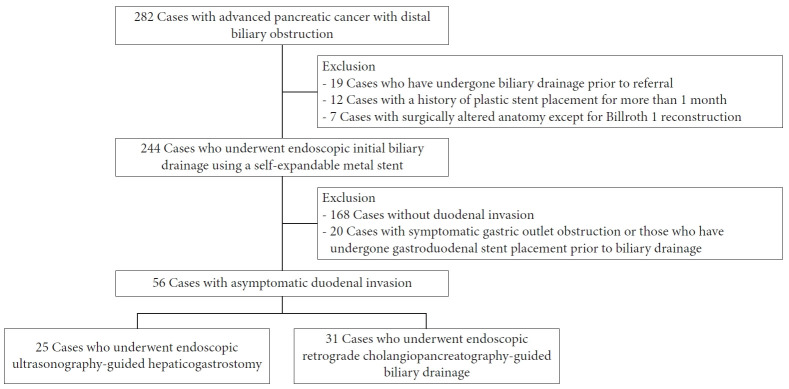
Methods: We enrolled 56 patients with pancreatic cancer and asymptomatic DI who underwent EUS-HGS (n=25) or ERCP-BD (n=31). Technical and clinical success, early (<3 months) and overall RBO rates, time to RBO (TRBO), and adverse events were compared between the EUS-HGS and ERCP-BD groups. Risk factors for early RBO were also evaluated.
Results: Baseline characteristics were similar between the groups. Both procedures demonstrated 100% technical and clinical success rates, with a similar incidence of adverse events (48% vs. 39%, p=0.59). While the median TRBO was comparable (5.7 vs. 8.8 months, p=0.60), EUS-HGS was associated with a lower incidence of early RBO compared to ERCP-BD (8% vs. 29%, p=0.09). The major causes of early RBO in ERCP-BD were sludge and food impaction, rarely occurring in EUS-HGS. EUS-HGS was potentially reduced early RBO (odds ratio, 0.32; p=0.07).
Conclusions: EUS-HGS can be a viable option for treating pancreatic cancer with asymptomatic DI.
Keywords: Duodenal invasion; Endoscopic retrograde cholangiopancreatography; Endoscopic ultrasound-guided hepaticogastrostomy; Malignant biliary obstruction; Pancreatic cancer.
Conflict of interest statement
Yousuke Nakai received research grants from Boston Scientific Japan, Fujifilm Corporation, and HOYA Corporation, and honoraria from Boston Scientific Japan, Fujifilm Corporation, Olympus Corporation, and Gadelius Medical. Mitsuhiro Fujishiro received research grants from Olympus Corporation and Fujifilm Corporation, and honoraria from Fujifilm Corporation and Olympus Corporation. The other authors declare no conflict of interest for this article.
Figures



Comment in
-
Biliary drainage in pancreatic cancer with duodenal invasion: which route is the best?Clin Endosc. 2025 Jan;58(1):82-84. doi: 10.5946/ce.2024.301. Epub 2025 Jan 24. Clin Endosc. 2025. PMID: 39895272 Free PMC article. No abstract available.
References
-
- Dumonceau JM, Tringali A, Papanikolaou IS, et al. Endoscopic biliary stenting: indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline: updated October 2017. Endoscopy. 2018;50:910–930. - PubMed
-
- Hamada T, Nakai Y, Isayama H, et al. Duodenal metal stent placement is a risk factor for biliary metal stent dysfunction: an analysis using a time-dependent covariate. Surg Endosc. 2013;27:1243–1248. - PubMed
-
- Hamada T, Isayama H, Nakai Y, et al. Duodenal invasion is a risk factor for the early dysfunction of biliary metal stents in unresectable pancreatic cancer. Gastrointest Endosc. 2011;74:548–555. - PubMed
-
- Giovannini M, Moutardier V, Pesenti C, et al. Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy. 2001;33:898–900. - PubMed
-
- Park DH, Jang JW, Lee SS, et al. EUS-guided biliary drainage with transluminal stenting after failed ERCP: predictors of adverse events and long-term results. Gastrointest Endosc. 2011;74:1276–1284. - PubMed
LinkOut - more resources
Full Text Sources
