

Anti-MDA5 autoantibodies predict clinical dynamics of dermatomyositis following SARS-CoV-2 mRNA vaccination: a retrospective statistical analysis of case reports
- PMID: 39190200
- PMCID: PMC11393189
- DOI: 10.1007/s00296-024-05683-5
Anti-MDA5 autoantibodies predict clinical dynamics of dermatomyositis following SARS-CoV-2 mRNA vaccination: a retrospective statistical analysis of case reports
Abstract
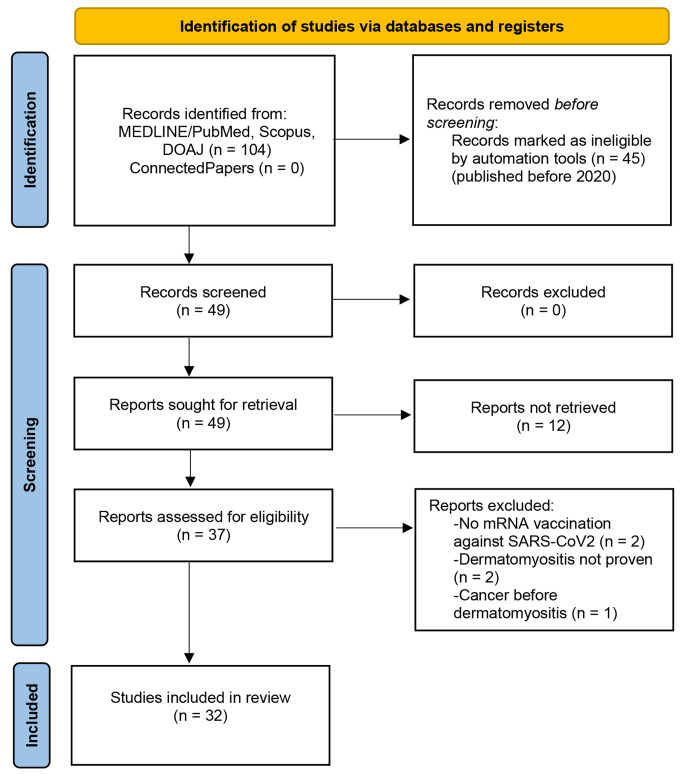
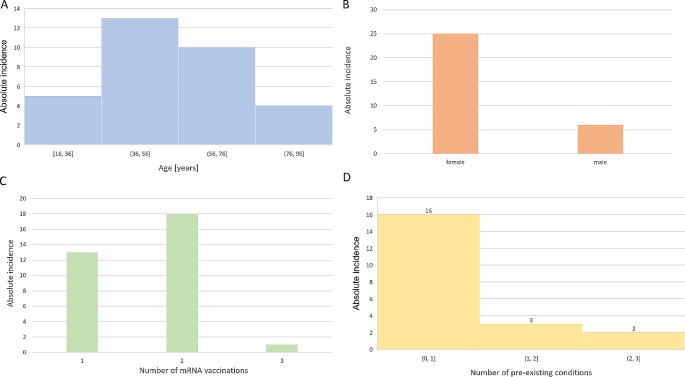
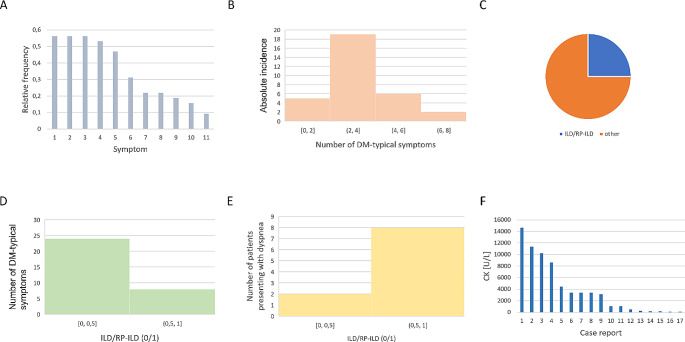
Since the introduction of mRNA vaccines against SARS-CoV-2, the induction of autoimmunity by mRNA vaccination has been discussed. Several cases of dermatomyositis (DM) associated with mRNA vaccination against SARS-CoV-2 infection have been reported. The question is whether there is a common pathomechanism for the induction of DM by this mRNA vaccination. The aim of this review is to analyse the sample of previously published case reports of DM following COVID-19 mRNA vaccination for common indicators of a possible immune pathomechanism.In this review, we summarised case reports of DM following mRNA vaccination against COVID-19. We considered this case report landscape as a cumulative sample (n = 32) and identified common clinical and molecular parameters in the intersection of case reports and statistically analysed the effect of these parameters on the development of DM.MDA-5 antibodies seem to play a role in the autoantibody signature after mRNA vaccination. MDA-5-positive DM is statistically more strongly associated with mRNA vaccination and interstitial lung disease/rapidly progressive interstitial lung disease (ILD/RP-ILD) than MDA-5-negative DM. MDA-5-positive DM seems not to be associated with an increased risk of malignancy, whereas MDA-5-negative DM is more strongly associated with malignancy.Our findings emphasize the potential role of innate antiviral signalling pathways in connecting DM to mRNA vaccination. MDA-5 autoantibodies appear to be predictive of a severe DM progression following mRNA vaccination. There seems to be an association between MDA-5 autoantibodies and paraneoplastic DM post-vaccination. Further studies are required to uncover the underlying mechanisms of autoimmunity triggered by mRNA vaccination.
Keywords: Autoimmunity; COVID-19; Case report; Dermatomyositis; MDA-5; mRNA vaccination.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interest.
Figures

References
-
- Mammen AL, Allenbach Y, Stenzel W, Benveniste O, Allenbach Y, Benveniste O et al (2020) 239th ENMC international workshop: classification of dermatomyositis, Amsterdam, the Netherlands, 14–16 December 2018. Neuromuscular Disorders. ;30:70–92. 10.1016/j.nmd.2019.10.005 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
