

Immunologic signatures of response and resistance to nivolumab with ipilimumab in advanced metastatic cancer
- PMID: 39190534
- PMCID: PMC11349049
- DOI: 10.1084/jem.20240152
Immunologic signatures of response and resistance to nivolumab with ipilimumab in advanced metastatic cancer
Abstract
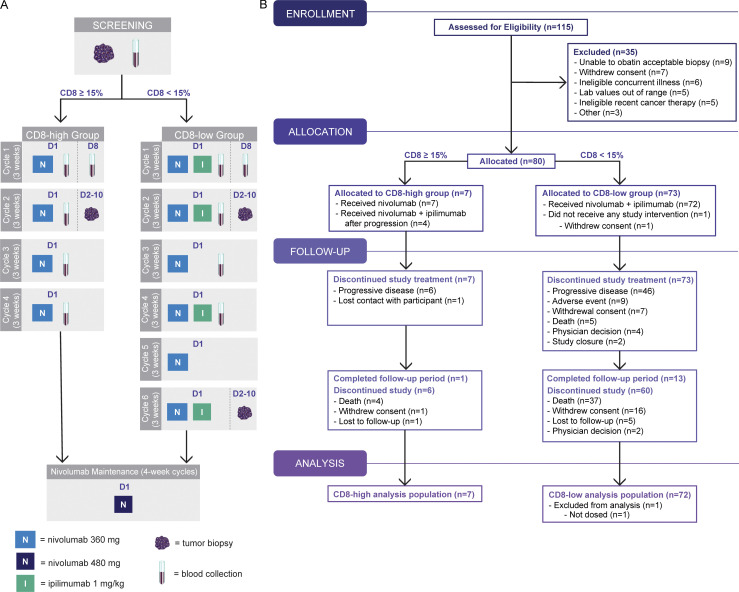
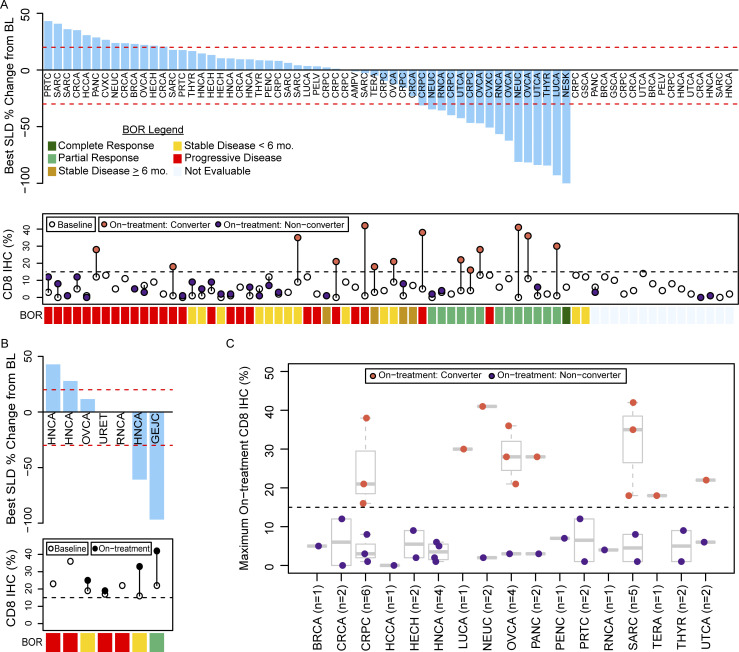
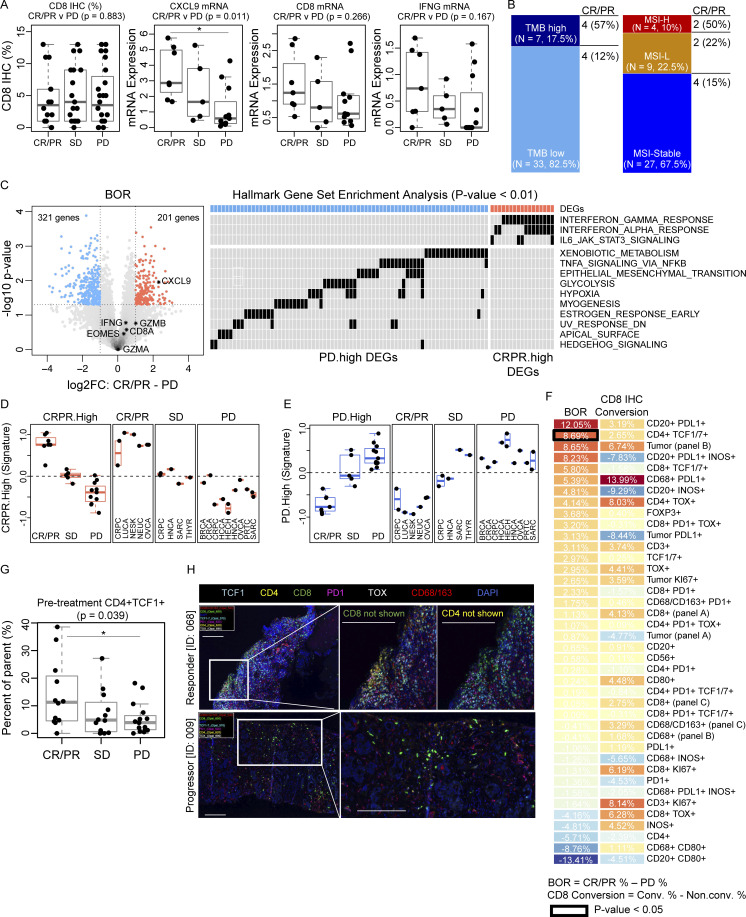
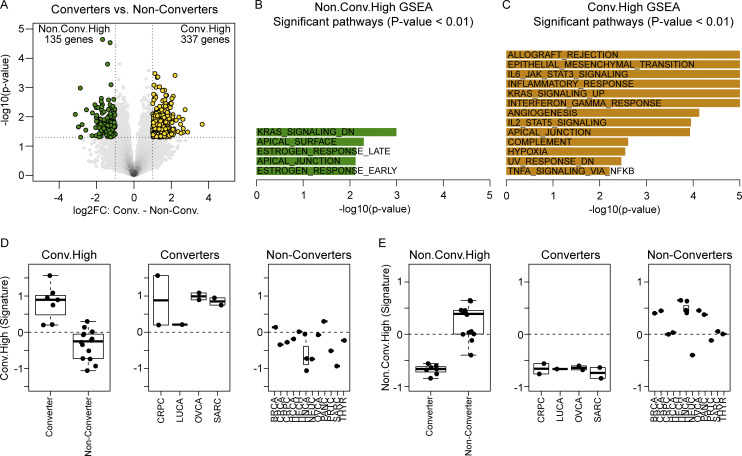
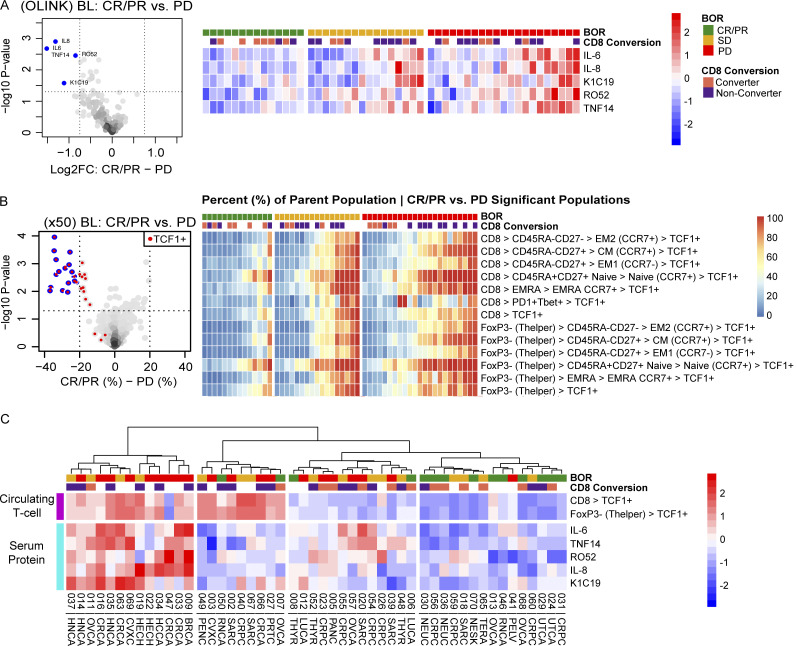
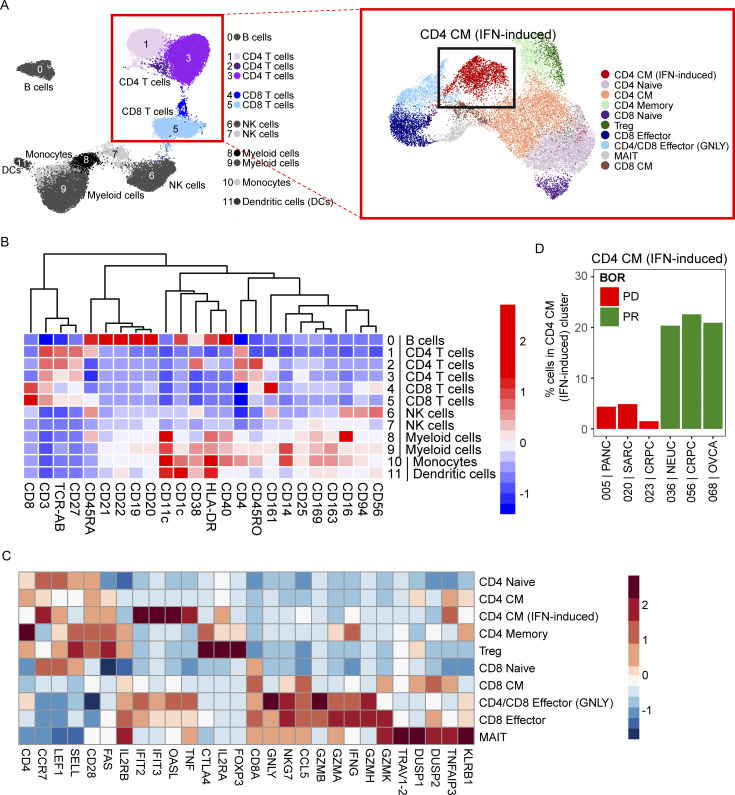
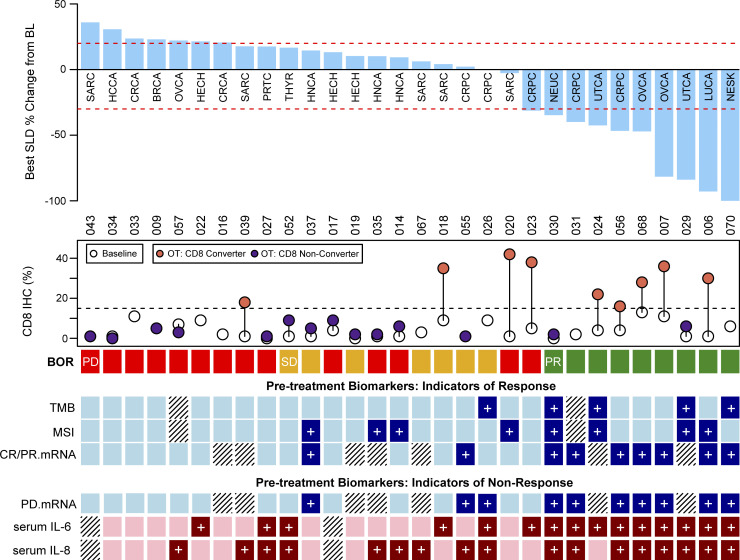
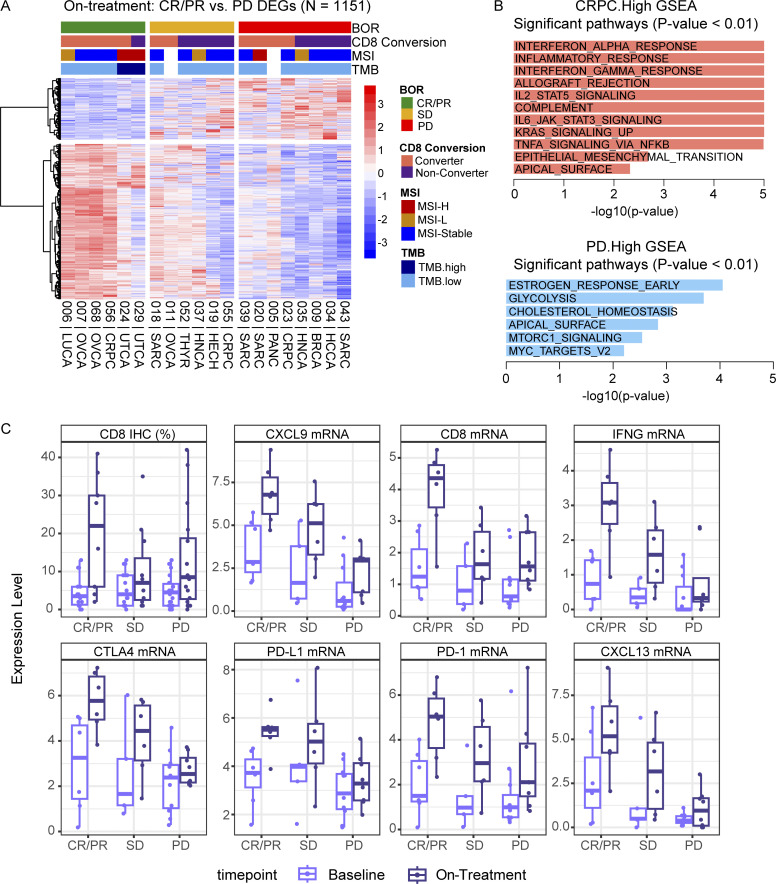
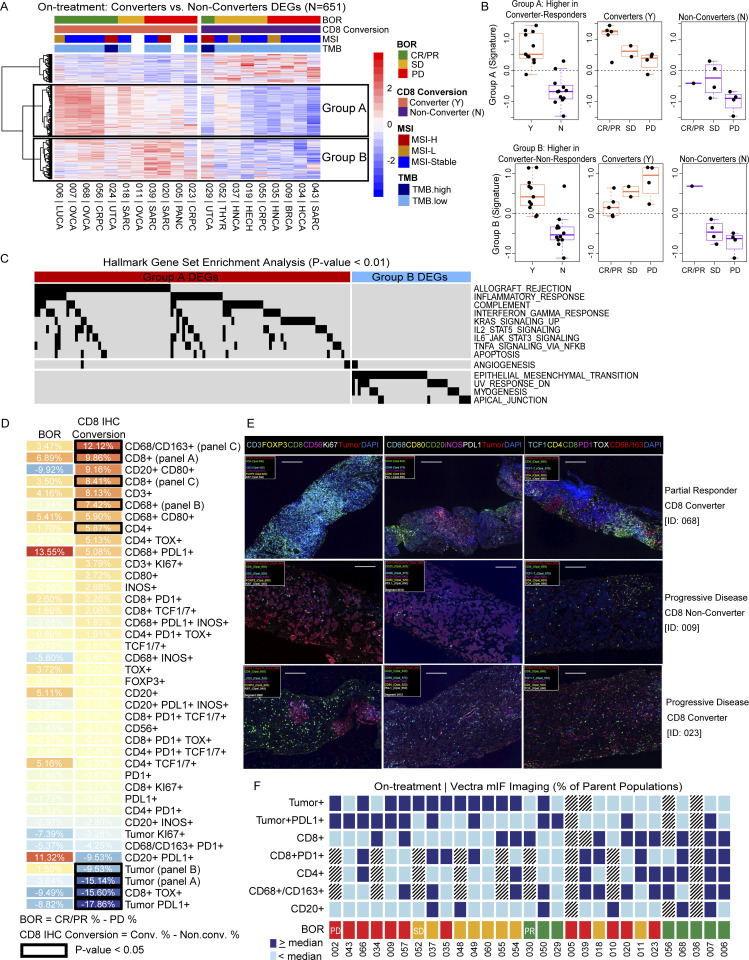
Identifying pan-tumor biomarkers that predict responses to immune checkpoint inhibitors (ICI) is critically needed. In the AMADEUS clinical trial (NCT03651271), patients with various advanced solid tumors were assessed for changes in intratumoral CD8 percentages and their response to ICI. Patients were grouped based on tumoral CD8 levels: those with CD8 <15% (CD8-low) received nivolumab (anti-PD-1) plus ipilimumab (anti-CTLA4) and those with CD8 ≥15% (CD8-high) received nivolumab monotherapy. 79 patients (72 CD8-low and 7 CD8-high) were treated. The disease control rate was 25.0% (18/72; 95% CI: 15.8-35.2) in CD8-low and 14.3% (1/7; 95% CI: 1.1-43.8) in CD8-high. Tumors from 35.9% (14/39; 95% CI: 21.8-51.4) of patients converted from CD8 <15% pretreatment to ≥15% after treatment. Multiomic analyses showed that CD8-low responders had an inflammatory tumor microenvironment pretreatment, enhanced by an influx of CD8 T cells, CD4 T cells, B cells, and macrophages upon treatment. These findings reveal crucial pan-cancer immunological features for ICI response in patients with metastatic disease.
© 2024 Tsimberidou et al.
Conflict of interest statement
Disclosures: A.M. Tsimberidou reported grants from Parker Institute for Cancer Immunotherapy (PICI) during the conduct of the study; grants from OBI Pharmaceuticals, Tachyon, Orionis, AbbVie, Immatics, Vividion, Novocure, Tempus, Agenus, Tvardi, and Macrogenics; and personal fees from Avstera, Macrogenics, BrYet, Bioeclipse, NEX-I, and VinceRx outside the submitted work. A. Drakaki reported personal fees from BMS, Merck, AZ, Roche, Seagen, Exelixis, and EMD Serono outside the submitted work. D.N. Khalil reported personal fees from Abbvie, Akamis Bio, and Celldex Therapeutics outside the submitted work; in addition, D.N. Khalil had a patent to US20240109973A1 pending, a patent to AU2016304597B2 issued, and a patent to CA3042867A1 pending. S. Kummar reported personal fees from Fortress Biotech, Inc., Gilead, GI Innovation, Inc., Mundibiopharma, Oxford Biotherapeutics, Springworks Therapeutics, Bayer, Genome Insight, XYOne Therapeutics, BPGbio Therapeutics, Genome and Company, and HarbourBiomed and “other” from Pathomiq and Mirati outside the submitted work. F.S. Hodi reported “other” from Bristol Myers Squibb during the conduct of the study and personal fees from Bristol Myers Squibb, Merck, Novartis, Compass Therapeutics, Apricity, 7 Hills Pharma, Bicara, Checkpoint Therapeutics, Genentech, Bioentre, Gossamer, Iovance, Catalym, Immunocore, Kairos, Rheos, Bayer, Zumotor, Corner Therapeutics, Puretech, Curis, Astra Zeneca, Pliant, Solu Therapeutics, Vir biotechnology, and 92Bio outside the submitted work; in addition, F.S. Hodi had a patent to Methods for Treating MICA-Related Disorders (#20100111973) with royalties paid to institution per institutional policies, a patent to Tumor antigens and uses thereof (#7250291) issued, a patent to Angiopoiten-2 Biomarkers Predictive of Anti-immune checkpoint response (#20170248603) pending, a patent to Compositions and Methods for Identification, Assessment, Prevention, and Treatment of Melanoma using PD-L1 Isoforms (#20160340407) pending, a patent to Therapeutic peptides (#20160046716) pending, a patent to Methods of Using Pembrolizumab and Trebananib pending, a patent to Vaccine compositions and methods for restoring NKG2D pathway function against cancers Patent number: 10279021 with royalties paid to institution per institutional, a patent to Antibodies that bind to MHC class I polypeptide-related sequence A Patent number: 10106611 with royalties paid to institution per institutional, a patent to Anti-Galectin Antibody Biomarkers Predictive of Anti-Immune Checkpoint and Anti-Angiogenesis Responses pending, and a patent to Antibodies against EDIL3 and methods of use thereof pending. D.Y. Oh reported grants from Damon Runyon Cancer Research Foundation, V Foundation for Cancer Research, Prostate Cancer Foundation, and Nutcracker Therapeutics; “other” from Merck, PACT Pharma, Poseida Therapeutics, TCR2 Therapeutics, and Roche/Genentech; and personal fees from Revelation Partners outside the submitted work; and has received research support (to the institution) from Merck, PACT Pharma, Poseida Therapeutics, TCR2 Therapeutics, Roche/Genentech, and Nutcracker Therapeutics; travel and accommodations from Roche/Genentech; and has consulted for Revelation Partners. M. Amouzgar reported fees for consulting. M. Spasic reported personal fees from Natera outside the submitted work. M.T. Tetzlaff reported “other” from Merck and personal fees from Clinical care options outside the submitted work. T.J. Hollmann reported grants from Bristol Myers Squibb, Calico Labs, and PICI during the conduct of the study. J.S. Moore reported, “This was performed on a flow cytometer provided to the Parker Institute for Cancer Immunotherapy and some panel reagents were provided under an agreement between BDIS and PICI.” S. Velichko reported personal fees from Natera, Inc. during the conduct of the study. S. Bucktrout reported personal fees from Akamis Bio outside the submitted work. U. Dugan reported “other” from BMS during the conduct of the study. At the time of writing this manuscript V.M. Hubbard-Lucey is employed and has stock/interest in Bristol Myers Squibb. J. O’Donnell-Tormey reported grants from Bristol Myers Squibb outside the submitted work. L.H. Butterfield reported advisory activities (honoraria): Calidi Scientific and Medical Advisory Board, 2017–2023; KaliVir, Scientific Advisory Board, 2018–2023; Torque Therapeutics, Scientific Advisory Board, 2018–2020; Khloris, Scientific Advisory Board, 2019–2023; Pyxis, Scientific Advisory Board, 2019–2023; CytomX, Scientific Advisory Board, 2019–2023; DCprime, Scientific Advisory Board meeting, Nov. 2020; RAPT, Scientific Advisory Board, 2020–2023; Takeda, Scientific Advisor, 2020–2023; EnaraBio scientific advisor, Feb. 2021; Federation Bio scientific advisor Sept.–Oct. 2022; Pfizer scientific advisor Oct. 2022, Apple Tree 2022–2023, Orionis 2023. J. Fairchild reported personal fees from PICI outside the submitted work. T.M. LaVallee reported personal fees from PICI outside the submitted work; and is currently employed at Coherus Biosciences. P. Sharma reported “other” from Achelois, Adaptive Biotechnologies, Affini-T, Akoya Biosciences, Apricity, Asher Bio, BioAtla LLC, BioNTech, Candel Therapeutics, Catalio, C-Reveal Therapeutics, Dragonfly Therapeutics, Earli Inc, Enable Medicine, Glympse, Henlius/Hengenix, Hummingbird, ImaginAb, InterVenn Biosciences, JSL Health, LAVA Therapeutics, Lytix Biopharma, Marker Therapeutics, Matrisome, Oncolytics, Osteologic, PBM Capital, Phenomic AI, Polaris Pharma, Sporos, Spotlight, Time Bioventures, Trained Therapeutix Discovery, Two Bear Capital, and Xilis, Inc. outside the submitted work. No other disclosures were reported.
Figures

References
-
- Assarsson, E., Lundberg M., Holmquist G., Björkesten J., Thorsen S.B., Ekman D., Eriksson A., Rennel Dickens E., Ohlsson S., Edfeldt G., et al. 2014. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS One. 9:e95192. 10.1371/journal.pone.0095192 - DOI - PMC - PubMed
-
- Beltra, J.-C., Manne S., Abdel-Hakeem M.S., Kurachi M., Giles J.R., Chen Z., Casella V., Ngiow S.F., Khan O., Huang Y.J., et al. 2020. Developmental relationships of four exhausted CD8+ T cell subsets reveals underlying transcriptional and epigenetic landscape control mechanisms. Immunity. 52:825–841.e8. 10.1016/j.immuni.2020.04.014 - DOI - PMC - PubMed
-
- Bratman, S.V., Yang S.Y.C., Iafolla M.A.J., Liu Z., Hansen A.R., Bedard P.L., Lheureux S., Spreafico A., Razak A.A., Shchegrova S., et al. 2020. Personalized circulating tumor DNA analysis as a predictive biomarker in solid tumor patients treated with pembrolizumab. Nat. Cancer. 1:873–881. 10.1038/s43018-020-0096-5 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
