

TRPA1 aggravates osteoclastogenesis and osteoporosis through activating endoplasmic reticulum stress mediated by SRXN1
- PMID: 39191723
- PMCID: PMC11349872
- DOI: 10.1038/s41419-024-07018-5
TRPA1 aggravates osteoclastogenesis and osteoporosis through activating endoplasmic reticulum stress mediated by SRXN1
Abstract
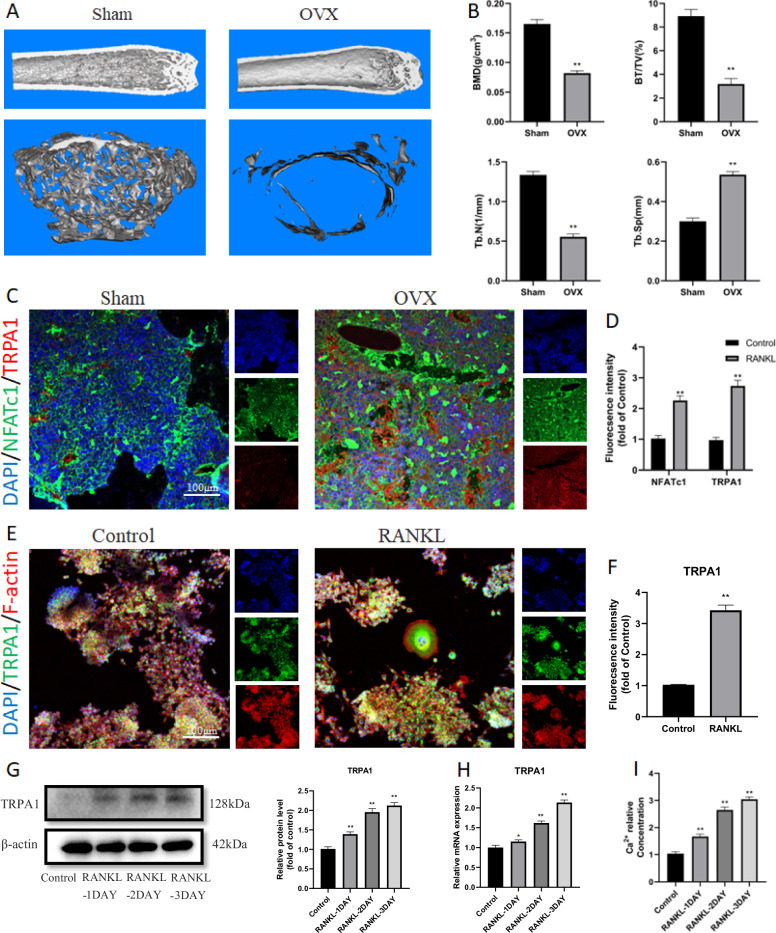
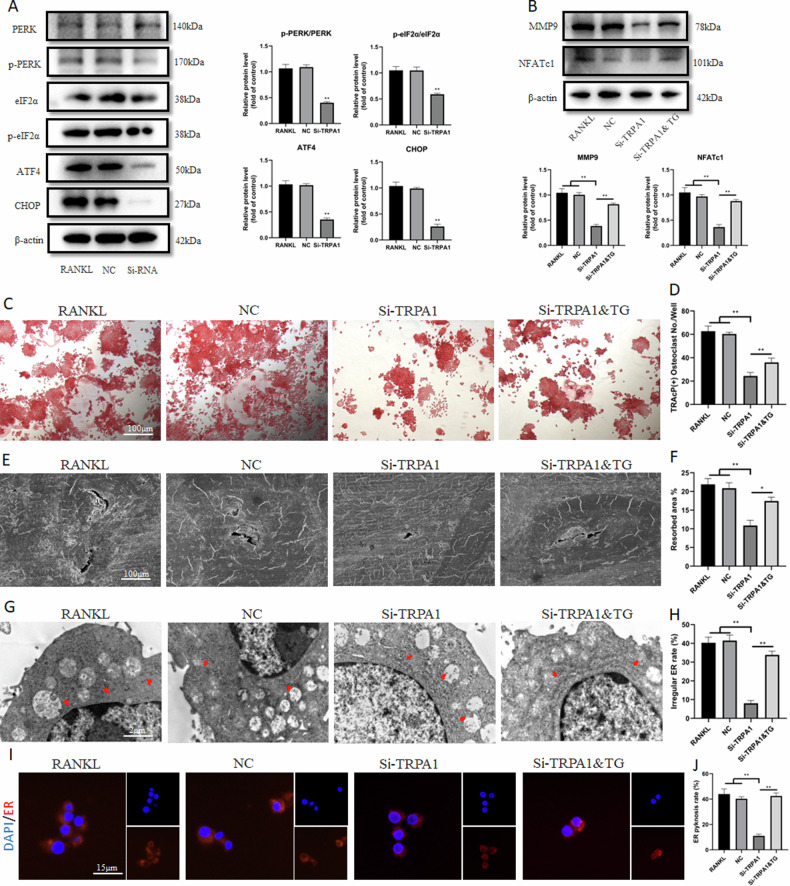
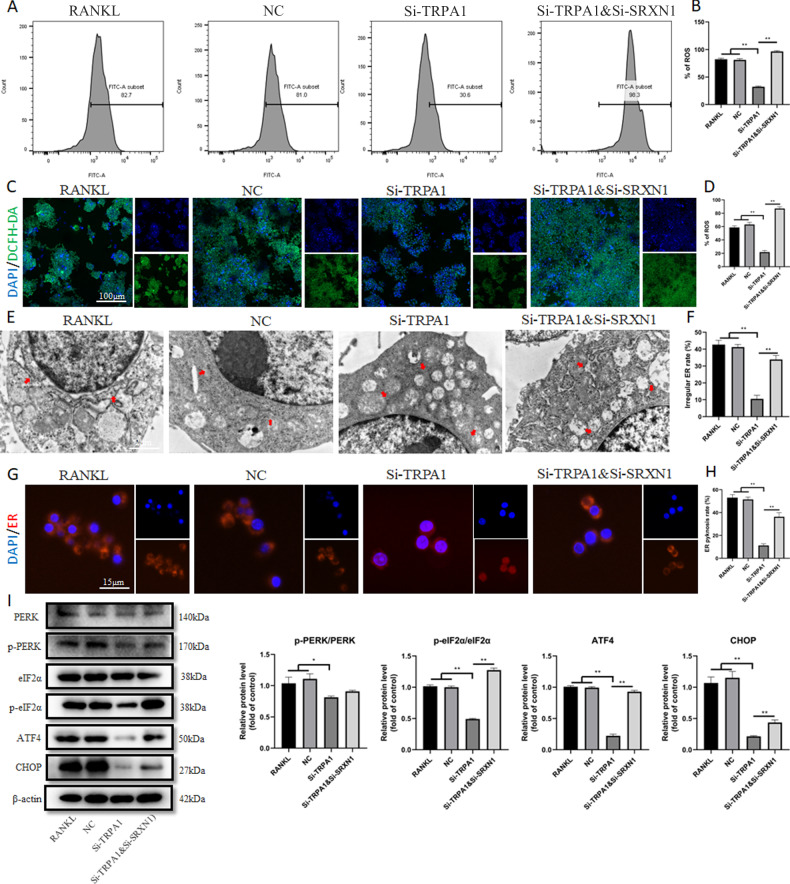
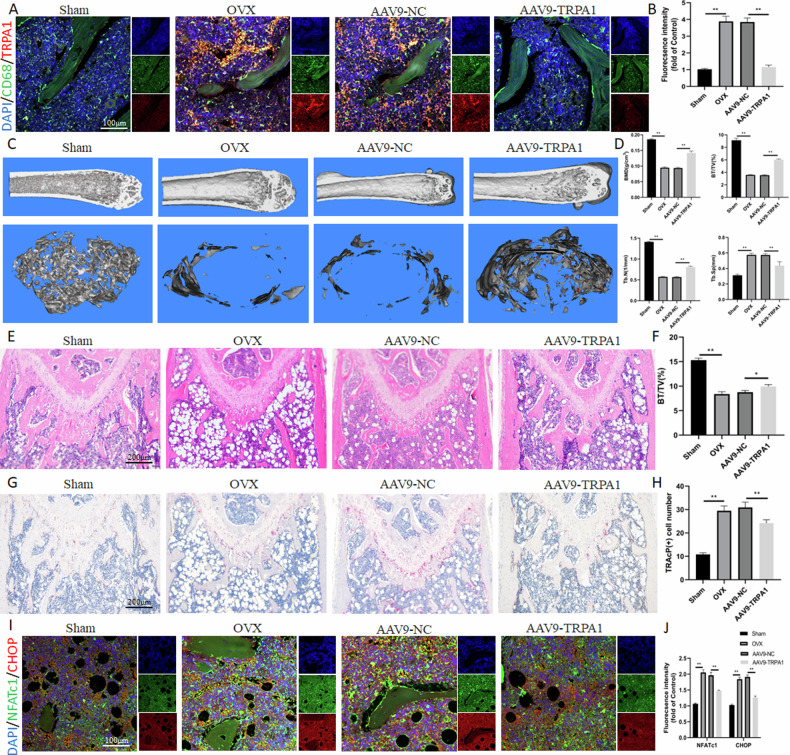
Osteoporosis (OP) is a disorder of bone remodeling caused by an imbalance between bone resorption by osteoclasts and bone formation by osteoblasts. Therefore, inhibiting excessive osteoclast activity is one of the promising strategies for treating OP. A major transient receptor potential cation channel, known as transient receptor potential ankyrin 1 (TRPA1), was found to alleviate joint pain and cartilage degeneration in osteoarthritis. However, little research has focused on TRPA1 function in OP. As a result, this study aimed to explore the TRPA1 characteristics and its potential therapeutic function during osteoclastogenesis. The TRPA1 expression gradually increased in the osteoclast differentiation process; however, its suppression with small interfering RNA and an inhibitor (HC030031) significantly controlled the osteoclast count and the expression of osteoclast characteristic genes. Its suppression also inhibited endoplasmic reticulum (ER) stress-related pancreatic ER kinase (PERK) pathways. An ER stress inhibitor (thapsigargin) reversed the down-regulated levels of ER stress and osteoclast differentiation by suppressing TRPA1. Transcriptome sequencing results demonstrated that TRPA1 negatively regulated reactive oxygen species (ROS) and significantly increased the expression of an antioxidant gene, SRXN1. The osteoclast differentiation and the levels of ER stress were enhanced with SRXN1 inhibition. Finally, TRPA1 knockdown targeting macrophages by adeno-associated virus-9 could relieve osteoclast differentiation and osteopenia in ovariectomized mice. In summary, silencing TRPA1 restrained osteoclast differentiation through ROS-mediated down-regulation of ER stress via inhibiting PERK pathways. The study also indicated that TRPA1 might become a prospective treatment target for OP.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
PERK controls bone homeostasis through the regulation of osteoclast differentiation and function.Cell Death Dis. 2020 Oct 13;11(10):847. doi: 10.1038/s41419-020-03046-z. Cell Death Dis. 2020. PMID: 33051453 Free PMC article.
-
Increased RANKL-mediated osteoclastogenesis by interleukin-1β and endoplasmic reticulum stress.Joint Bone Spine. 2014 Dec;81(6):520-6. doi: 10.1016/j.jbspin.2014.04.012. Epub 2014 Jun 20. Joint Bone Spine. 2014. PMID: 24956991
-
Endoplasmic Reticulum-Bound Transcription Factor CREBH Stimulates RANKL-Induced Osteoclastogenesis.J Immunol. 2018 Mar 1;200(5):1661-1670. doi: 10.4049/jimmunol.1701036. Epub 2018 Jan 29. J Immunol. 2018. PMID: 29378912
-
ER Stress, the Unfolded Protein Response and Osteoclastogenesis: A Review.Biomolecules. 2023 Jun 28;13(7):1050. doi: 10.3390/biom13071050. Biomolecules. 2023. PMID: 37509086 Free PMC article. Review.
-
Advances in the interaction between endoplasmic reticulum stress and osteoporosis.Biomed Pharmacother. 2023 Sep;165:115134. doi: 10.1016/j.biopha.2023.115134. Epub 2023 Jul 10. Biomed Pharmacother. 2023. PMID: 37437374 Review.
Cited by
-
NAD+/Nrf2 signaling promotes osteogenesis by regulating oxidative level of BMSCs under mechanical stress.Prog Orthod. 2025 May 30;26(1):19. doi: 10.1186/s40510-025-00566-2. Prog Orthod. 2025. PMID: 40445451 Free PMC article.
-
Srxn1 Overexpression Protect Against Cardiac Remodelling by Inhibiting Oxidative Stress and Inflammation.J Cell Mol Med. 2025 Mar;29(6):e70432. doi: 10.1111/jcmm.70432. J Cell Mol Med. 2025. PMID: 40111164 Free PMC article.
-
Role of TRP Channels in Cancer-Induced Bone Pain.Int J Mol Sci. 2025 Jan 30;26(3):1229. doi: 10.3390/ijms26031229. Int J Mol Sci. 2025. PMID: 39940997 Free PMC article. Review.
-
Molecular mechanisms and targeted therapy of progranulin in metabolic diseases.Front Endocrinol (Lausanne). 2025 Apr 11;16:1553794. doi: 10.3389/fendo.2025.1553794. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40290306 Free PMC article. Review.
References
-
- Imai K, Ohnishi I, Matsumoto T, Yamamoto S, Nakamura K. Assessment of vertebral fracture risk and therapeutic effects of alendronate in postmenopausal women using a quantitative computed tomography-based nonlinear finite element method. Osteoporos Int. 2009;20:801–10. 10.1007/s00198-008-0750-8 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
