

Plasma proteomics of acute tubular injury
- PMID: 39191768
- PMCID: PMC11349760
- DOI: 10.1038/s41467-024-51304-x
Plasma proteomics of acute tubular injury
Abstract
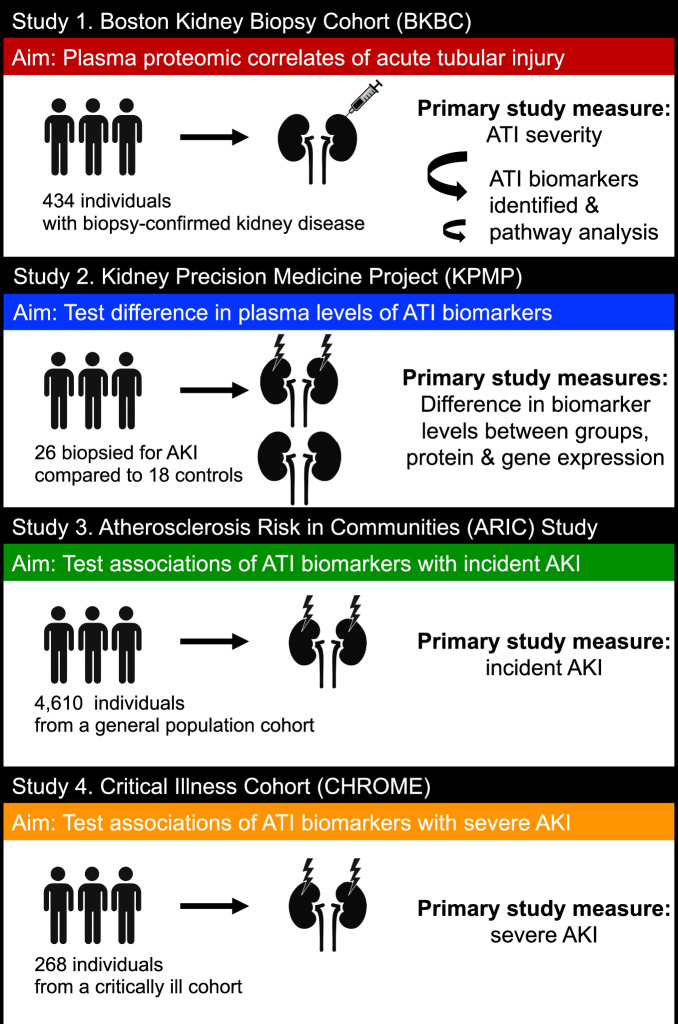
The kidney tubules constitute two-thirds of the cells of the kidney and account for the majority of the organ's metabolic energy expenditure. Acute tubular injury (ATI) is observed across various types of kidney diseases and may significantly contribute to progression to kidney failure. Non-invasive biomarkers of ATI may allow for early detection and drug development. Using the SomaScan proteomics platform on 434 patients with biopsy-confirmed kidney disease, we here identify plasma biomarkers associated with ATI severity. We employ regional transcriptomics and proteomics, single-cell RNA sequencing, and pathway analysis to explore biomarker protein and gene expression and enriched biological pathways. Additionally, we examine ATI biomarker associations with acute kidney injury (AKI) in the Kidney Precision Medicine Project (KPMP) (n = 44), the Atherosclerosis Risk in Communities (ARIC) study (n = 4610), and the COVID-19 Host Response and Clinical Outcomes (CHROME) study (n = 268). Our findings indicate 156 plasma proteins significantly linked to ATI with osteopontin, macrophage mannose receptor 1, and tenascin C showing the strongest associations. Pathway analysis highlight immune regulation and organelle stress responses in ATI pathogenesis.
© 2024. The Author(s).
Conflict of interest statement
S.S.W. reports personal fees from Public Health Advocacy Institute, CVS, Roth Capital Partners, Kantum Pharma, Mallinckrodt, Wolters Kluewer, GE Health Care, GSK, Allena Pharmaceuticals, Mass Medical International, Barron and Budd (vs Fresenius), JNJ, Venbio, Strataca, Takeda, Cerus, Pfizer, Bunch and James, Harvard Clinical Research Institute (aka Baim), Oxidien, Sironax, Metro Biotechnology, Biomarin, and Bain. S.E.R reports grant support to Joslin from Bayer and AstraZeneca. In addition, she has participated as advisory member for Bayer and AstraZeneca. D.G.M. is named co-inventor on a pending patent, “Methods and Systems for Diagnosis of Acute Interstitial Nephritis” and is a co-founder of the diagnostics company Predict AIN, LLC. Y.W. reports being an employee of Genentech and having stock and stock options in Roche at the time of final manuscript revision. The remaining authors declare that they have no competing interests.
Figures



References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
