

Prospective comparative analysis of three types of decompressive surgery for lumbar central stenosis: conventional, full-endoscopic, and biportal endoscopic laminectomy
- PMID: 39191792
- PMCID: PMC11349896
- DOI: 10.1038/s41598-024-65923-3
Prospective comparative analysis of three types of decompressive surgery for lumbar central stenosis: conventional, full-endoscopic, and biportal endoscopic laminectomy
Abstract
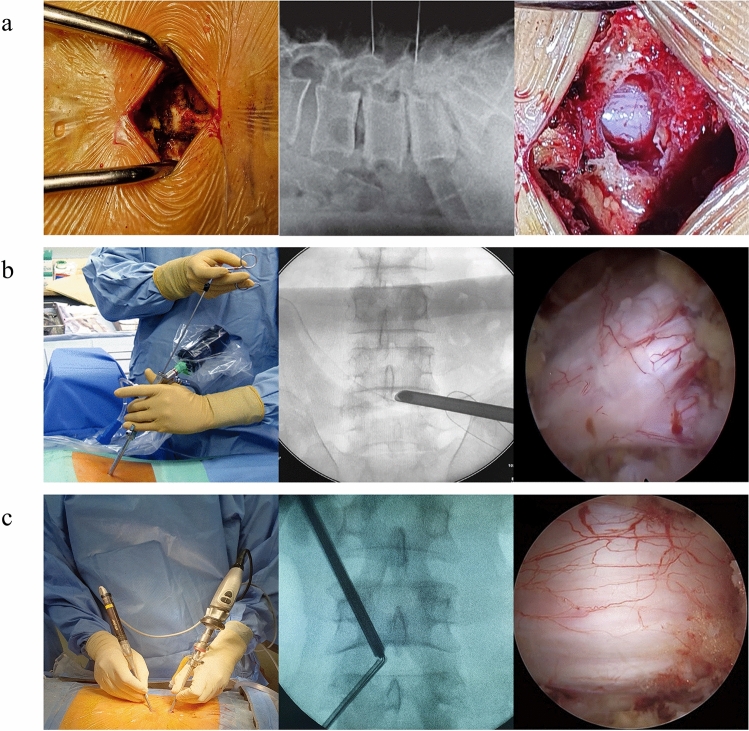
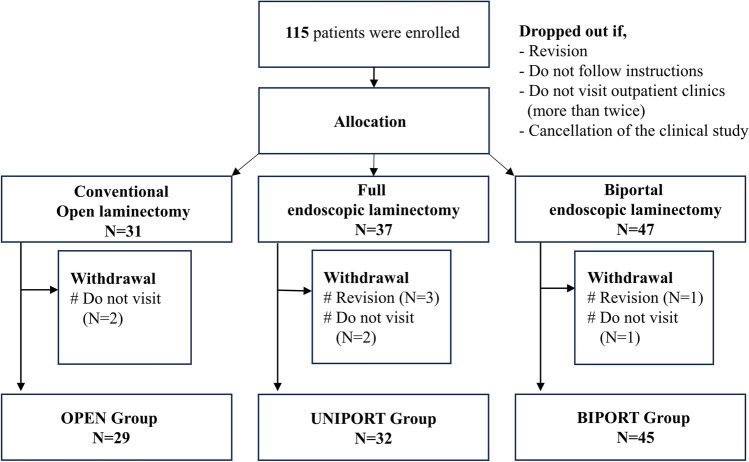
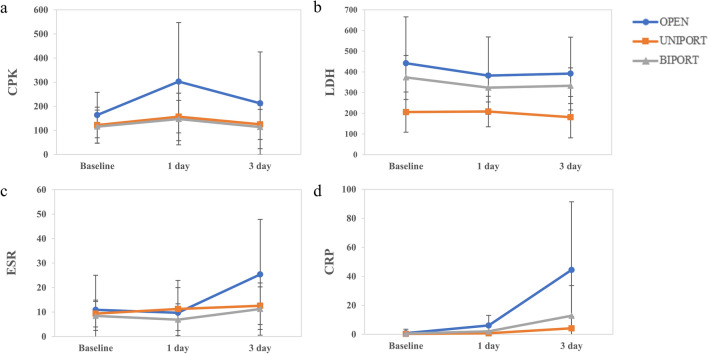
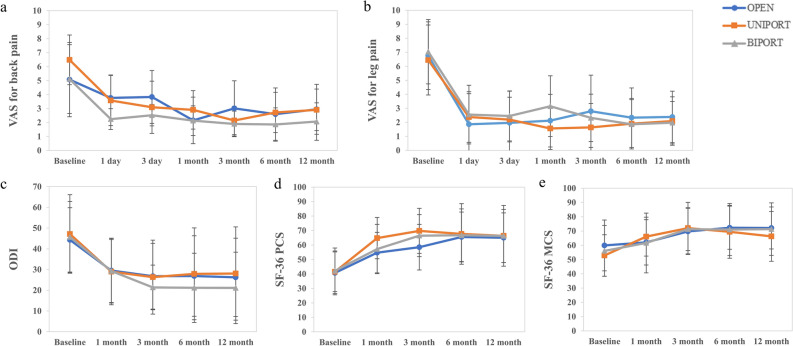
Conventional open laminectomy has long been considered one of the important surgical options for lumbar central stenosis owing to its positive outcomes. However, newer approaches have emerged as alternatives, including full-endoscopic and biportal endoscopic laminectomy. Therefore, a comparison of the outcomes that are associated with each of these surgical methods is warranted. This prospective multicenter trial, initiated in February 2019, compared the outcomes of three lumbar central stenosis surgical approaches: open laminectomy (OPEN), uniportal endoscopy (UNIPORT), and biportal endoscopy (BIPORT). Among 115 participants from seven centers, one-year follow-ups assessed laboratory, radiological, and clinical outcomes. Despite all groups showing adequate decompression and clinical improvement, the OPEN group exhibited less improvement in Visual analog scale (VAS) for back pain scores (p < 0.05) and significant postoperative increases in most laboratory markers. Furthermore, the OPEN group experienced a significant decrease in multifidus muscle cross-sectional area compared to endoscopic groups (p < 0.001). Each surgical techniques produced similar clinical outcomes and dural space expansion. However, endoscopic surgery was associated with better muscle preservation and better relief of back pain. Endoscopic surgery is a reasonable alternative to conventional laminectomy for treating lumbar central stenosis.This trial was registered on CRIS (Clinical Research Information Service, KCT0004355).
© 2024. The Author(s).
Conflict of interest statement
The study was supported primarily by research funds from the Korean Spinal Neurosurgery Society (KSNS). The funding organization was not involved in any aspect of the trial, including study design, data analysis, or results interpretation. Partial support for patient follow-up examination expenses. All authors declare no personal conflicts of interest.
Figures

References
-
- Parker, S. L. et al. Two-year comprehensive medical management of degenerative lumbar spine disease (lumbar spondylolisthesis, stenosis, or disc herniation): A value analysis of cost, pain, disability, and quality of life. J. Neurosurg. Spine21, 143–149 (2014). 10.3171/2014.3.SPINE1320 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
