

Retrospective ANalysis of multi-drug resistant Gram-nEgative bacteRia on veno-venous extracorporeal membrane oxygenation. The multicenter RANGER STUDY
- PMID: 39192287
- PMCID: PMC11351604
- DOI: 10.1186/s13054-024-05068-x
Retrospective ANalysis of multi-drug resistant Gram-nEgative bacteRia on veno-venous extracorporeal membrane oxygenation. The multicenter RANGER STUDY
Erratum in
-
Correction to: Retrospective ANalysis of multi-drug resistant Gram-nEgative bacteRia on veno-venous extracorporeal membrane oxygenation. The multicenter RANGER STUDY.Crit Care. 2025 Feb 13;29(1):75. doi: 10.1186/s13054-024-05231-4. Crit Care. 2025. PMID: 39948680 Free PMC article. No abstract available.
Abstract
Background: Veno-venous extracorporeal membrane oxygenation (V-V ECMO) is a rapidly expanding life-support technique worldwide. The most common indications are severe hypoxemia and/or hypercapnia, unresponsive to conventional treatments, primarily in cases of acute respiratory distress syndrome. Concerning potential contraindications, there is no mention of microbiological history, especially related to multi-drug resistant (MDR) bacteria isolated before V-V ECMO placement. Our study aims to investigate: (i) the prevalence and incidence of MDR Gram-negative (GN) bacteria in a cohort of V-V ECMOs; (ii) the risk of 1-year mortality, especially in the case of predetected MDR GN bacteria; and (iii) the impact of annual hospital V-V ECMO volume on the probability of acquiring MDR GN bacteria.
Methods: All consecutive adults admitted to the Intensive Care Units of 5 Italian university-affiliated hospitals and requiring V-V ECMO were screened. Exclusion criteria were age < 18 years, pregnancy, veno-arterial or mixed ECMO-configuration, incomplete records, survival < 24 h after V-V ECMO. A standard protocol of microbiological surveillance was applied and MDR profiles were identified using in vitro susceptibility tests. Cox-proportional hazards models were applied for investigating mortality.
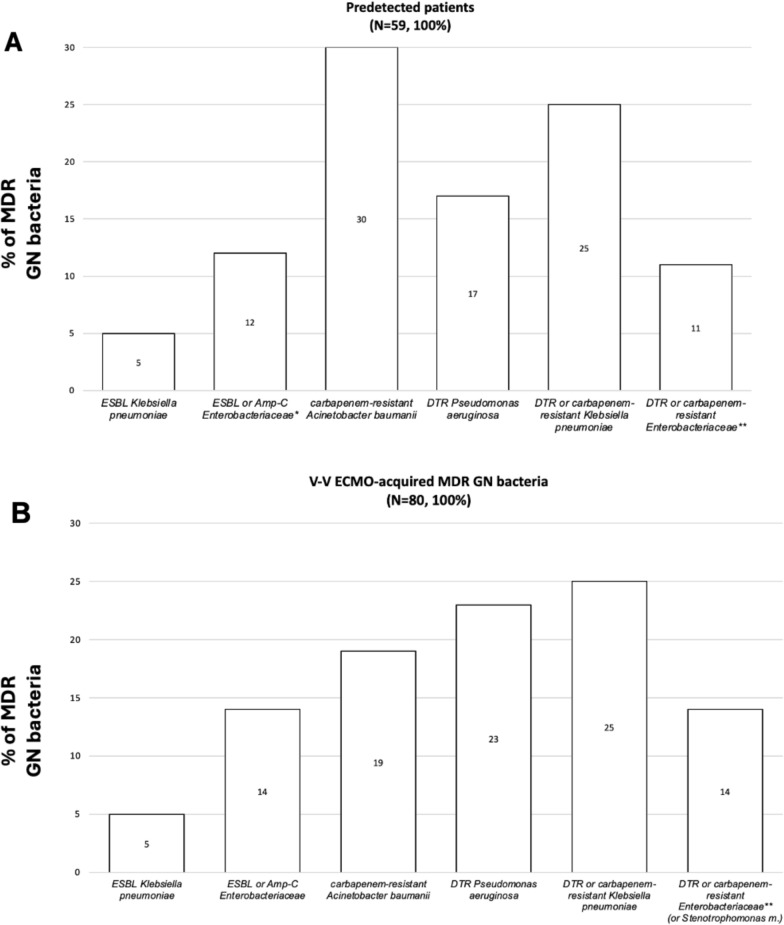
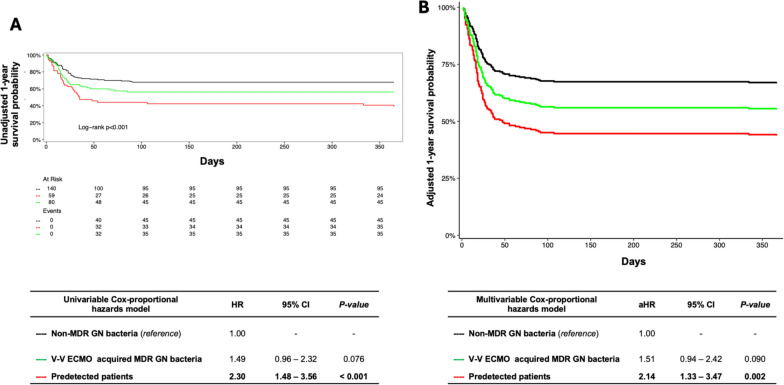
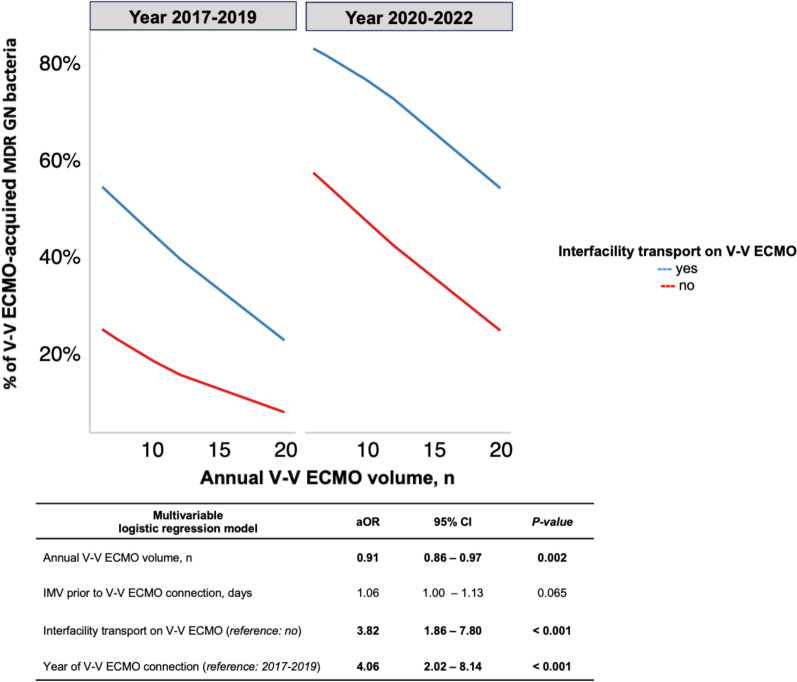
Results: Two hundred and seventy-nine V-V ECMO patients (72% male) were enrolled. The overall MDR GN bacteria percentage was 50%: 21% (n.59) detected before and 29% (n.80) after V-V ECMO placement. The overall 1-year mortality was 42%, with a higher risk observed in predetected patients (aHR 2.14 [1.33-3.47], p value 0.002), while not in 'V-V ECMO-acquired MDR GN bacteria' group (aHR 1.51 [0.94-2.42], p value 0.090), as compared to 'non-MDR GN bacteria' group (reference). Same findings were found considering only infections. A larger annual hospital V-V ECMO volume was associated with a lower probability of acquiring MDR GN bacteria during V-V ECMO course (aOR 0.91 [0.86-0.97], p value 0.002).
Conclusions: 21% of MDR GN bacteria were detected before; while 29% after V-V ECMO connection. A history of MDR GN bacteria, isolated before V-V ECMO, was an independent risk factor for mortality. The annual hospital V-V ECMO volume affected the probability of acquiring MDR GN bacteria. Trial Registration ClinicalTrial.gov Registration Number NCTNCT06199141, date 12.26.2023.
Keywords: ECMO; ESBL; Extended-spectrum beta-lactamase; Extracorporeal membrane oxygenation; MDR; MDRO; Multi-drug resistant.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Tonna JE, Abrams D, Brodie D, Greenwood JC, Rubio Mateo-Sidron JA, Usman A, et al. Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): guideline from the extracorporeal life support organization (ELSO). ASAIO J Am Soc Artif Intern Organs. 2021;67(6):601–10. - PMC - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. - PubMed
-
- Definition Task Force ARDS, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–33. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
