

Leaky Gut Syndrome: Myths and Management
- PMID: 39193076
- PMCID: PMC11345991
Leaky Gut Syndrome: Myths and Management
Abstract
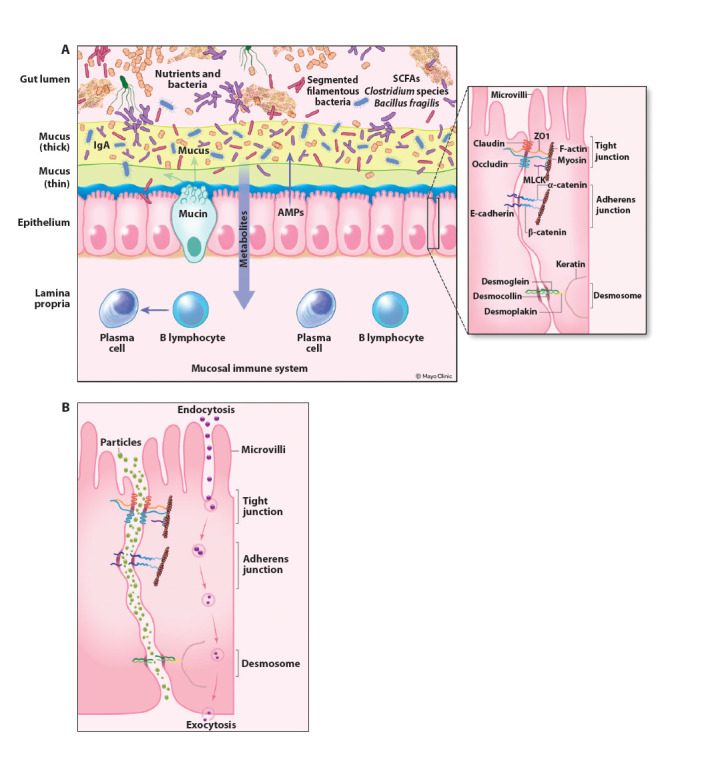
Leaky gut syndrome is a condition widely popularized in the lay literature, although it is not currently accepted as a formal medical diagnosis. Multiple gastrointestinal symptoms are ascribed to leaky gut syndrome, including diarrhea, bloating, distension, abdominal pain, and dyspeptic symptoms of early satiety, nausea, and postprandial fullness. The etiology and pathophysiology of leaky gut syndrome are multifactorial; a preceding gastrointestinal infection, inflammatory bowel disease, and certain medications may be relevant factors in some patients. The diagnosis of leaky gut syndrome is problematic. Although patients are frequently informed that the diagnosis can be readily made using results from blood work or stool studies, no validated test currently exists to make this diagnosis. Patients report a variety of myths about the etiology, diagnosis, and treatment of leaky gut syndrome, which can cause alarm and can frequently lead to expensive, unnecessary tests and unproven, sometimes dangerous treatments. This article reviews some of the most common myths about leaky gut syndrome and provides data from the scientific literature to correct these statements. Management strategies, based on data, are provided when available.
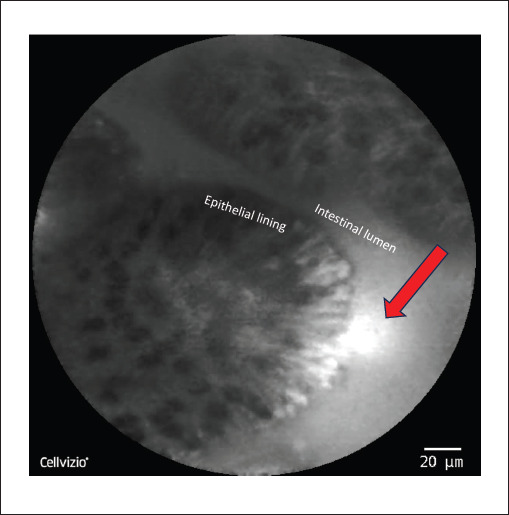
Keywords: Bloating; confocal laser endomicroscopy; glutamine; intestinal permeability; leaky gut syndrome; tight junctions.
Copyright © 2024, Gastro-Hep Communications, Inc.
Figures
References
-
- Osler W. The Principles and Practice of Medicine. 1892. New York, NY: Appleton & Co.
-
- D’Eufemia P, Celli M, Finocchiaro R et al. Abnormal intestinal permeability in children with autism. Acta Paediatr. 1996;85(9):1076–1079. - PubMed
LinkOut - more resources
Full Text Sources