

eHealth and mHealth in Antimicrobial Stewardship to Reduce Mortality in Empirical Antimicrobial Therapy and a Systematic Review with a Meta-Analysis of Adequate Therapy
- PMID: 39195005
- PMCID: PMC11353792
- DOI: 10.3390/idr16040054
eHealth and mHealth in Antimicrobial Stewardship to Reduce Mortality in Empirical Antimicrobial Therapy and a Systematic Review with a Meta-Analysis of Adequate Therapy
Abstract
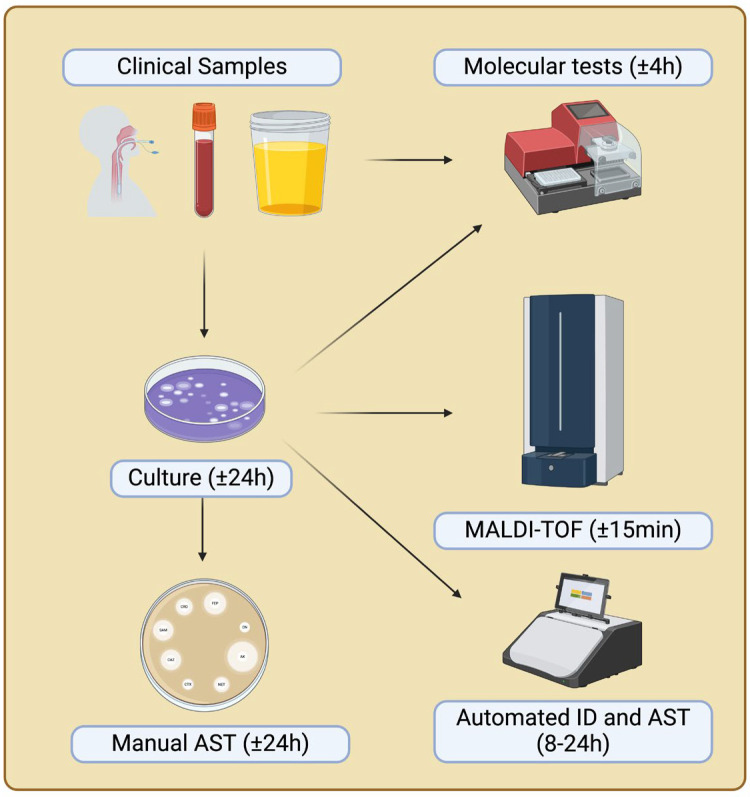
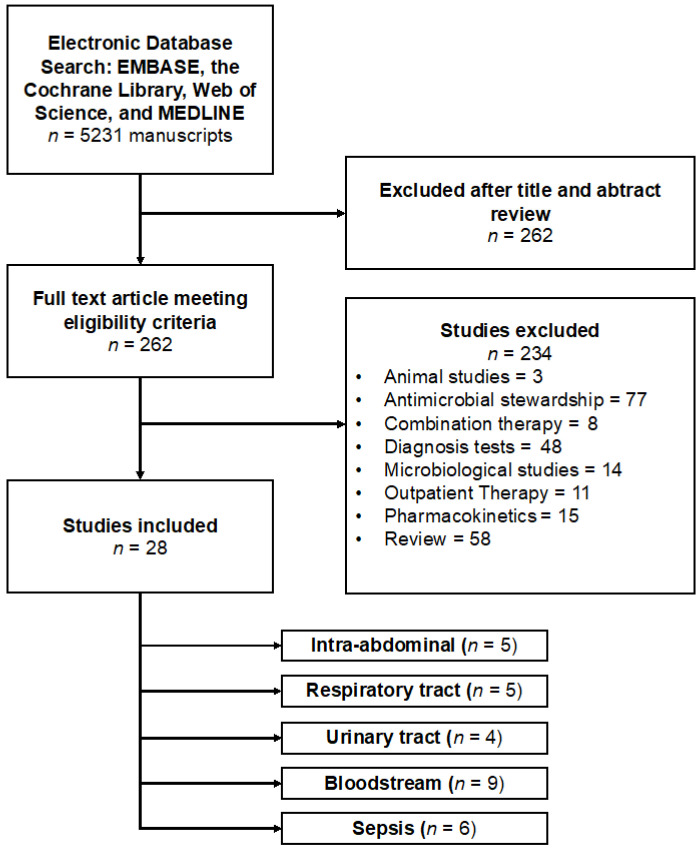
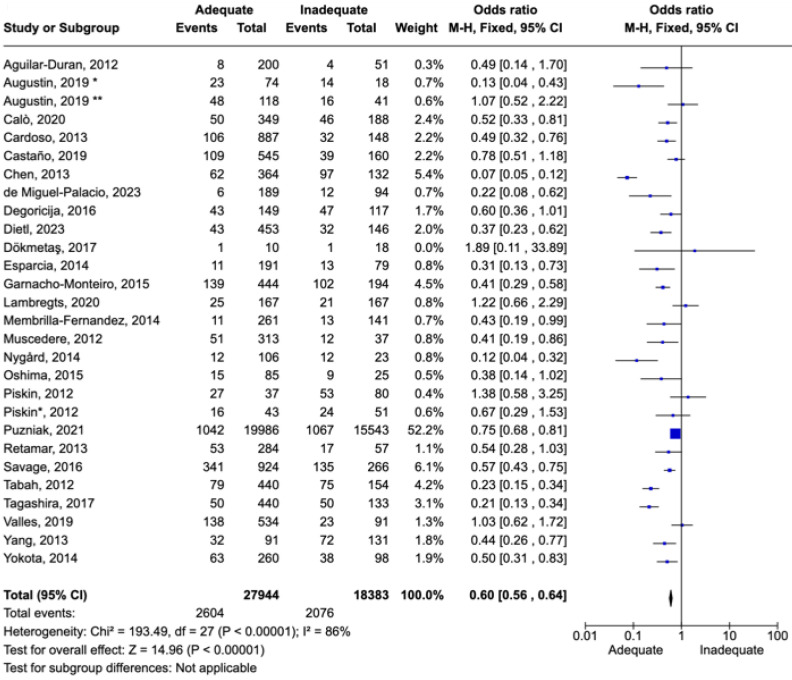
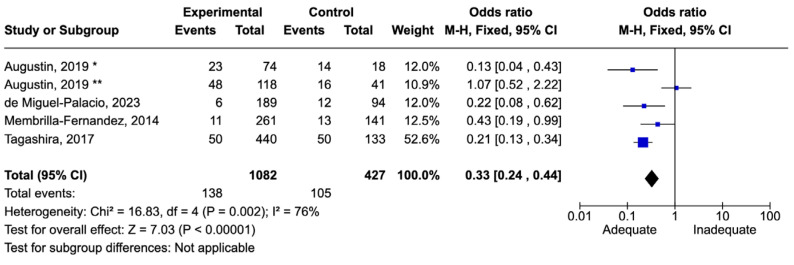
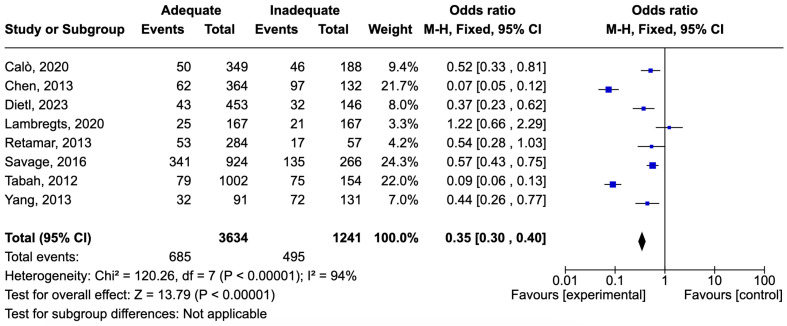
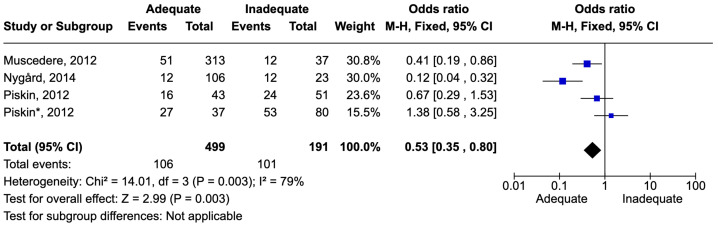
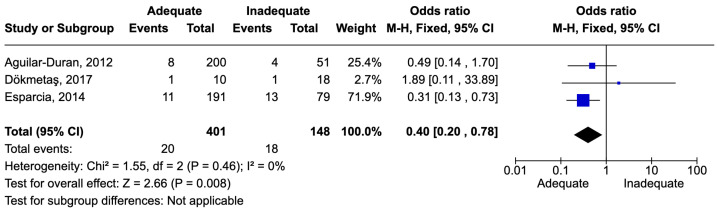
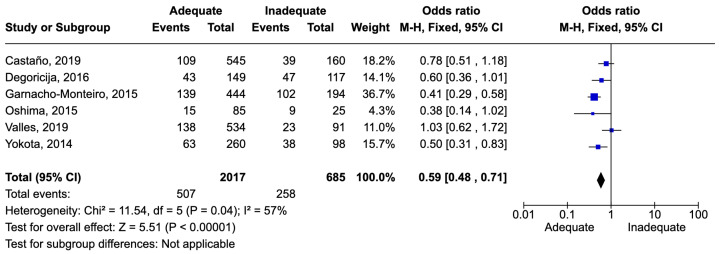
The urgent requirement for swift diagnostic methods in pathogen identification and antimicrobial susceptibility testing is emphasized by rising bacterial resistance and limited treatment options, which are particularly critical in sepsis management. The shift from traditional phenotype-based methods to rapid molecular and mass spectrometry techniques has significantly reduced result turnaround times, enhancing patient outcomes. In this systematic review with meta-analysis, the aspects of correct empirical antimicrobial therapy are evaluated to determine their impact on mortality. We performed a systematic review and meta-analysis on EMBASE, the Cochrane Library, Web of Science, and MEDLINE. Studies evaluating mortality associated with empirical adequate and inadequate therapy in different sites of infection were included. Outcomes included clinical cures in microbiologically evaluable patients. Among the sites of infection, the most studied were bloodstream infections (n = 9), followed by respiratory tract infections (n = 5), intra-abdominal infections (n = 5), and urinary tract infections (evaluated by 3 studies). Inadequate therapy was associated with an increase in mortality between 11 and 68%. Technologies to speed up pathogen identification are extremely necessary to reduce mortality.
Keywords: antimicrobial resistance; antimicrobial stewardship; eHealth; mHealth; pharmacotherapeutic algorithms; rapid diagnostic methods.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
eHealth and mHealth in Antimicrobial Stewardship Programs.Digit Biomark. 2024 Sep 20;8(1):194-206. doi: 10.1159/000541120. eCollection 2024 Jan-Dec. Digit Biomark. 2024. PMID: 39473804 Free PMC article. Review.
-
Cost Analysis of Implementing Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry Plus Real-Time Antimicrobial Stewardship Intervention for Bloodstream Infections.J Clin Microbiol. 2016 Dec 28;55(1):60-67. doi: 10.1128/JCM.01452-16. Print 2017 Jan. J Clin Microbiol. 2016. PMID: 27795335 Free PMC article.
-
Light Scattering Technology and MALDI-TOF MS in the microbiological fast-track of bloodstream infections: potential impact on antimicrobial treatment choices in a real-life setting.J Med Microbiol. 2023 Jan;72(1). doi: 10.1099/jmm.0.001638. J Med Microbiol. 2023. PMID: 36748537
-
Rapid versus standard antimicrobial susceptibility testing to guide treatment of bloodstream infection.Cochrane Database Syst Rev. 2021 May 4;5(5):CD013235. doi: 10.1002/14651858.CD013235.pub2. Cochrane Database Syst Rev. 2021. PMID: 34097767 Free PMC article.
-
Rates, predictors and mortality of community-onset bloodstream infections due to Pseudomonas aeruginosa: systematic review and meta-analysis.Clin Microbiol Infect. 2019 Aug;25(8):964-970. doi: 10.1016/j.cmi.2019.04.005. Epub 2019 Apr 14. Clin Microbiol Infect. 2019. PMID: 30995530
Cited by
-
Advances in Regenerative and Reconstructive Medicine in the Prevention and Treatment of Bone Infections.Biology (Basel). 2024 Aug 10;13(8):605. doi: 10.3390/biology13080605. Biology (Basel). 2024. PMID: 39194543 Free PMC article. Review.
-
Antimicrobial stewardship reduces antibiotic use density and cost in a Chinese tertiary hospital.Sci Rep. 2025 Jul 2;15(1):23609. doi: 10.1038/s41598-025-06622-5. Sci Rep. 2025. PMID: 40604070 Free PMC article.
References
-
- Wenzler E., Maximos M., Asempa T.E., Biehle L., Schuetz A.N., Hirsch E.B. Antimicrobial susceptibility testing: An updated primer for clinicians in the era of antimicrobial resistance: Insights from the Society of Infectious Diseases Pharmacists. Pharmacotherapy. 2023;43:264–278. doi: 10.1002/phar.2781. - DOI - PubMed
-
- Oteo J., Ortega A., Bartolome R., Bou G., Conejo C., Fernandez-Martinez M., Gonzalez-Lopez J.J., Martinez-Garcia L., Martinez-Martinez L., Merino M., et al. Prospective multicenter study of carbapenemase-producing Enterobacteriaceae from 83 hospitals in Spain reveals high in vitro susceptibility to colistin and meropenem. Antimicrob. Agents Chemother. 2015;59:3406–3412. doi: 10.1128/AAC.00086-15. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
