

Markers of imminent myocardial infarction
- PMID: 39196201
- PMCID: PMC11357982
- DOI: 10.1038/s44161-024-00422-2
Markers of imminent myocardial infarction
Abstract
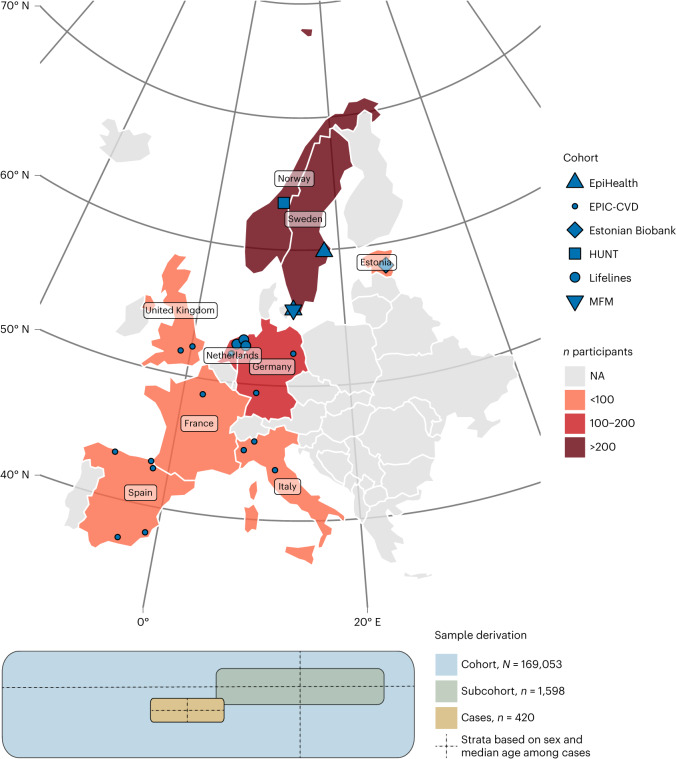
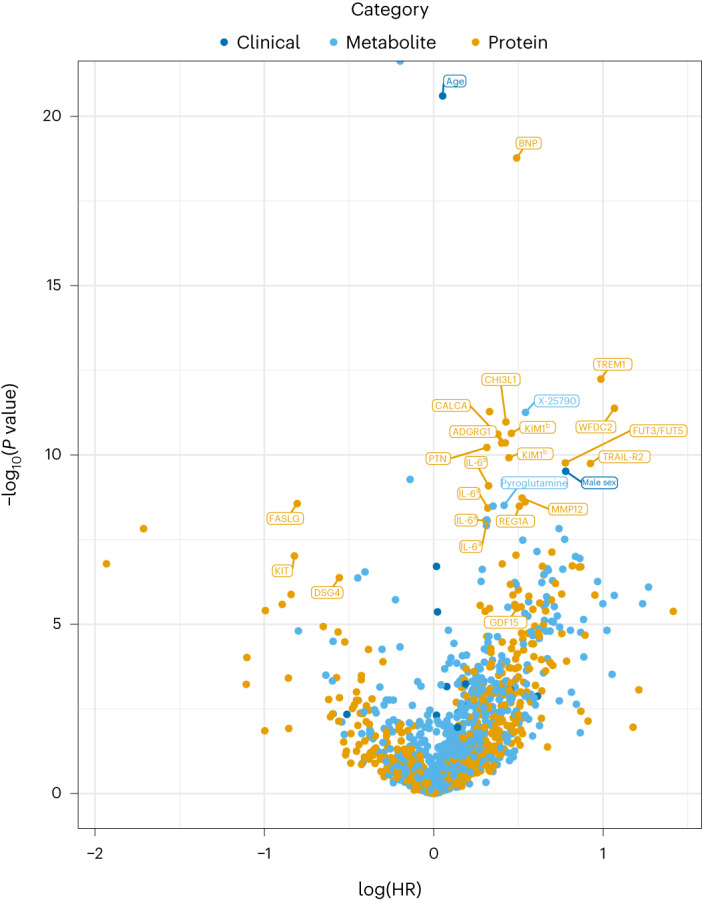
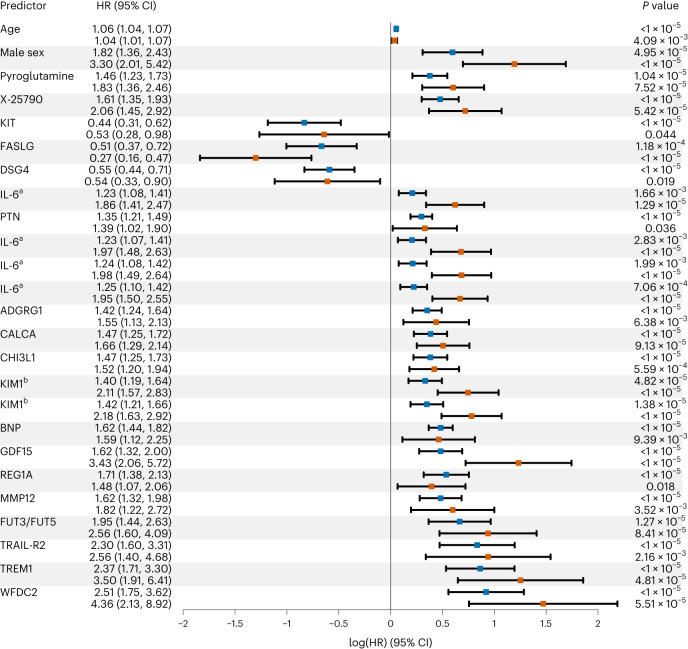
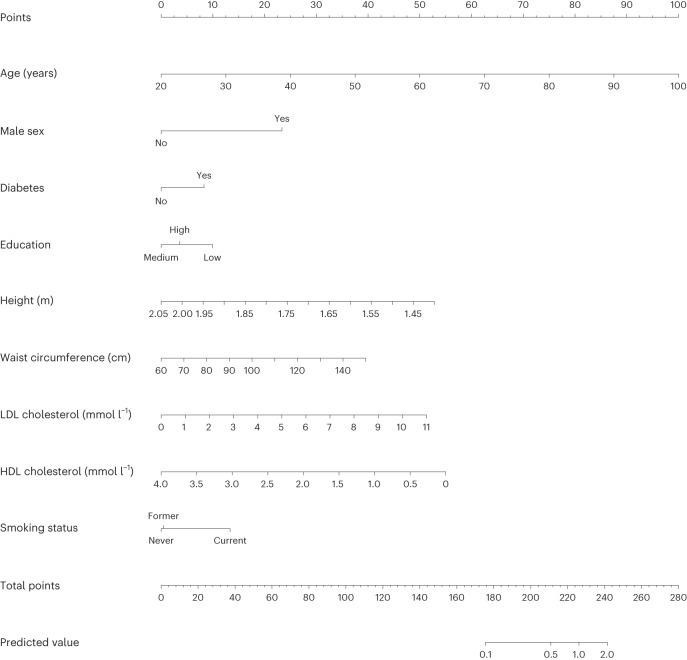
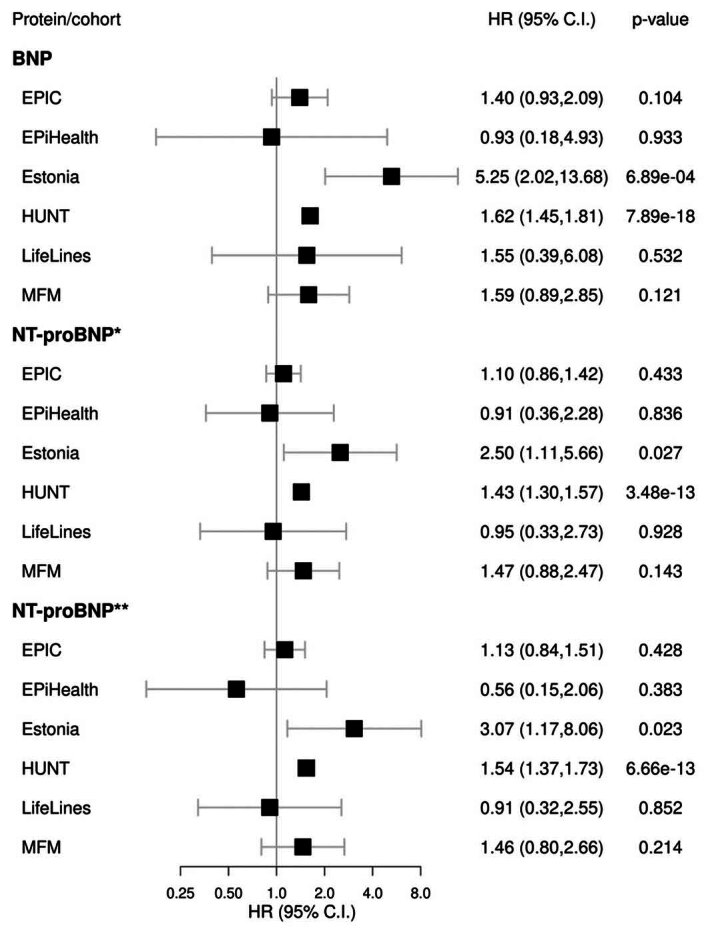
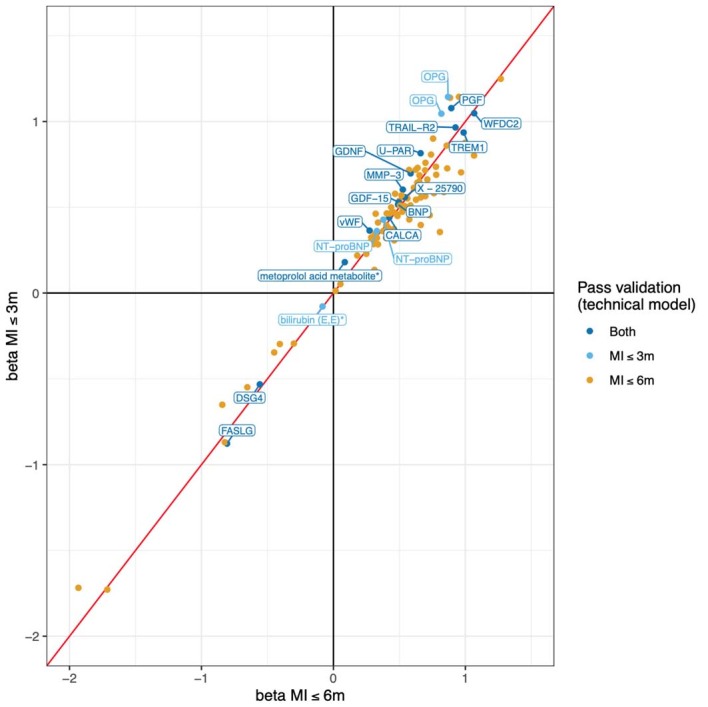
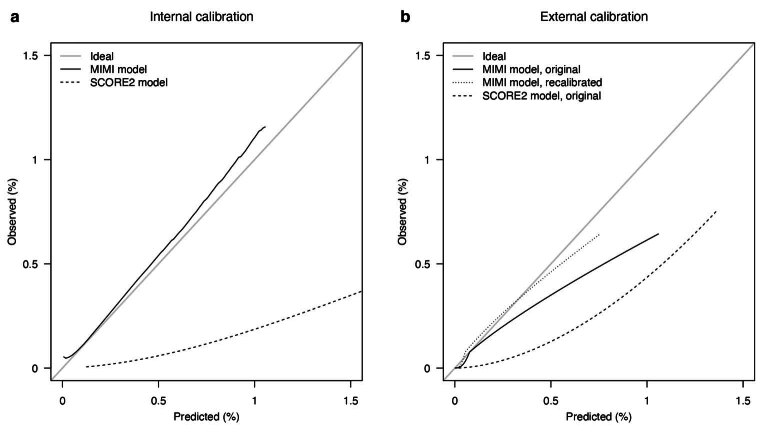
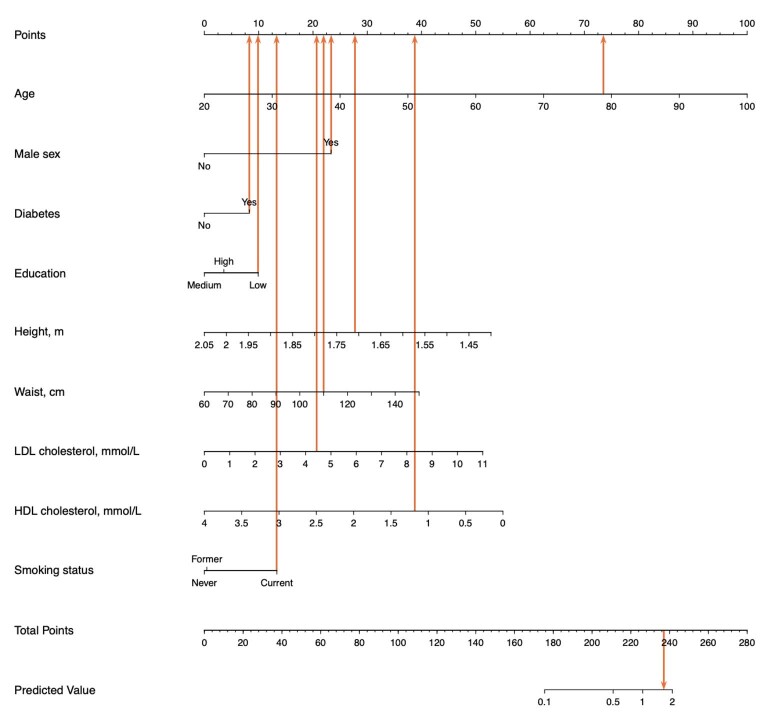
Myocardial infarction is a leading cause of death globally but is notoriously difficult to predict. We aimed to identify biomarkers of an imminent first myocardial infarction and design relevant prediction models. Here, we constructed a new case-cohort consortium of 2,018 persons without prior cardiovascular disease from six European cohorts, among whom 420 developed a first myocardial infarction within 6 months after the baseline blood draw. We analyzed 817 proteins and 1,025 metabolites in biobanked blood and 16 clinical variables. Forty-eight proteins, 43 metabolites, age, sex and systolic blood pressure were associated with the risk of an imminent first myocardial infarction. Brain natriuretic peptide was most consistently associated with the risk of imminent myocardial infarction. Using clinically readily available variables, we devised a prediction model for an imminent first myocardial infarction for clinical use in the general population, with good discriminatory performance and potential for motivating primary prevention efforts.
© 2024. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: A.S.B. reports grants outside this work (from AstraZeneca, Bayer, Biogen, BioMarin, Bioverativ, Novartis and Sanofi) and personal fees from Novartis. E.I. is now an employee at GlaxoSmithKline. S.G. is an employee of Sence Research AB. J.S. reports stock ownership in Anagram kommunikation AB and Symptoms Europe AB outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Challenges and opportunities for biomarker discovery to predict imminent myocardial infarction.Nat Cardiovasc Res. 2024 Feb;3(2):102-103. doi: 10.1038/s44161-024-00424-0. Nat Cardiovasc Res. 2024. PMID: 39196200 No abstract available.
References
-
- European Society of Cardiology, European Heart Network, European Commission, World Health Organization. European heart health charter. Eur. J. Prev. Cardiol. 10.1097/01.hjr.0000266926.91914.2a (2007).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical