

Spinal arteriovenous fistula leading to acute paraplegia after a lumbar nerve root block: Successful embolization with complete neurological recovery-a case report
- PMID: 39196273
- PMCID: PMC11569799
- DOI: 10.1177/15910199241276578
Spinal arteriovenous fistula leading to acute paraplegia after a lumbar nerve root block: Successful embolization with complete neurological recovery-a case report
Abstract
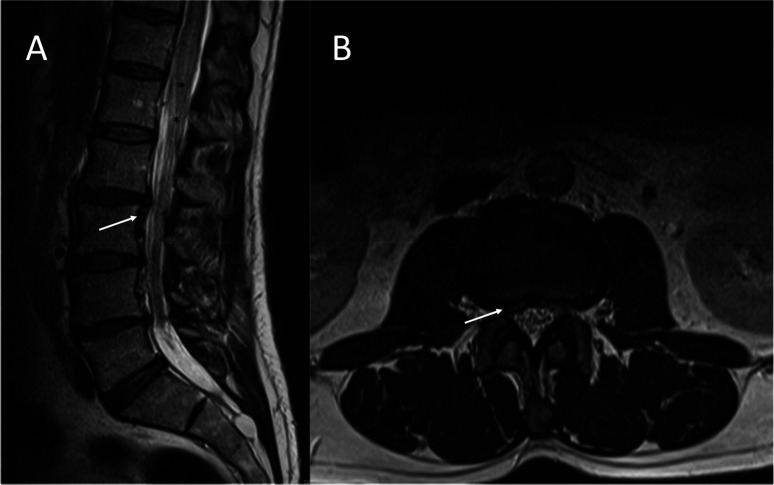
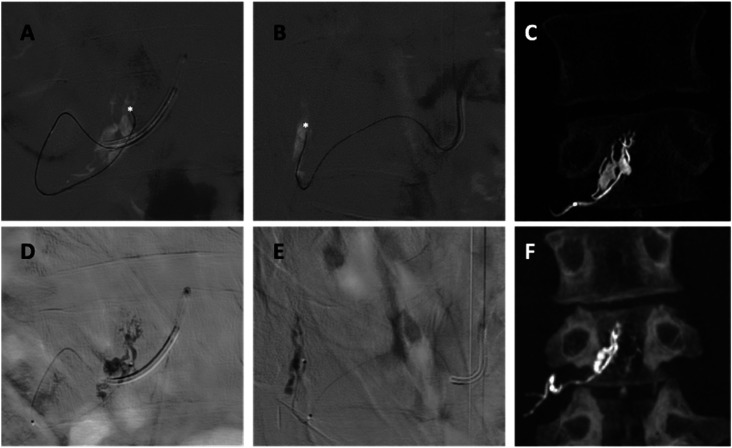
Spinal arteriovenous fistulas (SAVFs) are the most common type of vascular malformation of the spine in adult patients. They can lead to acute or progressive myelopathy due to venous congestion of the medullary veins. While most SAVFs are acquired, their pathophysiology remains unclear. The natural history of the disease and its clinical presentation are highly influenced by the location of the fistula and various factors may trigger sudden neurological decline. We present a case of a patient who developed a complete spinal cord injury after a lumbar nerve root block, likely due to an undiagnosed SAVF. The patient underwent endovascular embolization, resulting in a complete recovery of neurological function.
Keywords: Angiography; arteriovenous fistula; dural fistula; spine.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures




References
-
- Petrin Z, Marino RJ, Oleson CV, et al. Paralysis after lumbar interlaminar epidural steroid injection in the absence of hematoma: A case of congestive myelopathy due to spinal dural arteriovenous Fistula and a review of the literature. Am J Phys Med Rehabil 2020; 99: e107–e110. - PubMed
-
- International Spine Intervention Society. In: Bogduk N. (ed) ISIS practice guidelines for spinal diagnostic and treatment procedures, 2nd ed. San Francisco: International Spine Intervention Society, 2013.
-
- Geibprasert S, Pereira V, Krings T, et al. Dural arteriovenous shunts: A new classification of craniospinal epidural venous anatomical bases and clinical correlations. Stroke 2008; 39: 2783–2794. - PubMed
LinkOut - more resources
Full Text Sources
