

Hoffa's fat pad resection during total knee arthroplasty does not affect functioning and gait: a double-blind randomized clinical trial
- PMID: 39196403
- PMCID: PMC11417071
- DOI: 10.1007/s00402-024-05503-2
Hoffa's fat pad resection during total knee arthroplasty does not affect functioning and gait: a double-blind randomized clinical trial
Abstract
Introduction: Hoffa's fat pad is considered a source of anterior knee pain and may limit prosthetic knee function. Resection of Hoffa's fat pad in total knee arthroplasty (TKA), however, is controversial, and little is known about the functional outcomes including gait quality. This double-blind randomized controlled trial (i) compared functional recovery between TKAs where Hoffa was resected or preserved, and (ii) compared recovery of self-reported function with objective (gait-related) outcomes.
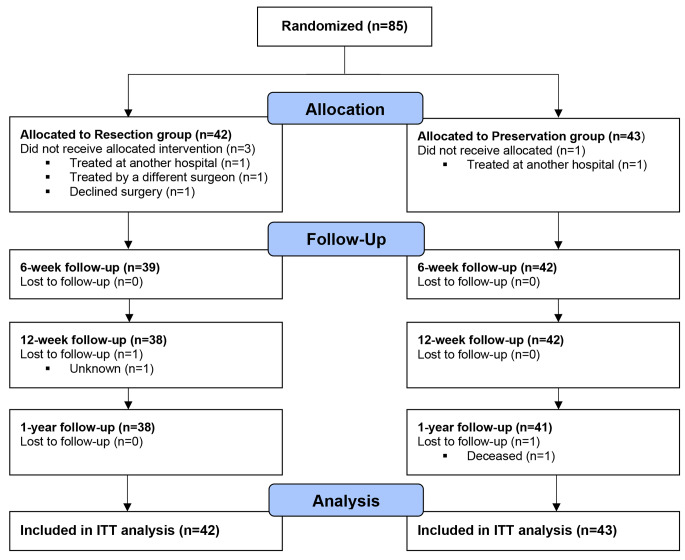
Materials and methods: Eighty-five patients (age 66.4 ± 8.0 years, 47% women) scheduled to undergo TKA for primary osteoarthritis were randomly assigned to either fat pad resection or preservation. Subjective measures of functioning were assessed at baseline, 6 weeks, 3 months, and 12 months postoperatively and included the Knee Injury and Osteoarthritis Outcome Score (KOOS), Kujala, and visual analog scale (VAS) for pain. Objective measures of functioning were assessed at baseline, 3 months, and 12 months postoperatively and included instrumented range-of-motion and gait analysis. Longitudinal analyses (generalized estimating equations) were used to compare recovery between groups, and chi-square tests compared attainment of minimal clinical important difference (MCID) and patient acceptable symptom state (PASS). Finally, correlation analyses explored associations between subjective and objective recovery in function.
Results: Resection patients showed poorer improvement in KOOS quality of life in the first 6 weeks (B=-10.02, 95% confidence interval (CI) [-18.91, -1.12], p = .027), but stronger improvement in knee extension after 3 months (B = 3.02, 95%CI [0.45, 5.60], p = .021) compared to preservation patients. Regarding MCID or PASS, no differences were noted between groups at 3 and 12 months (all p > .05). Subjective function substantially improved in the first 3 months, while objective outcomes improved only between 3 and 12 months. Moderate to strong correlations were identified between changes in knee flexion and gait with Kujala and KOOS in the resection but not in the preservation group.
Conclusions: Similar functional outcomes were achieved after TKA with or without resection of Hoffa's fat pad. Hence, removing the fat pad to promote surgical exposure will not affect functional outcomes including gait quality. Functional recovery of objective outcomes was not always consistent with subjective recovery, suggesting that both self-reported as well as objective, gait-related outcomes may provide meaningful information on functional recovery following TKA.
Trial registration: This clinical trial was prospectively registered under the Netherlands Trial Registry (# NL3638). This registry has recently been replaced by the Dutch Trial Registry where this study can be accessed via https://onderzoekmetmensen.nl/en/trial/20994 .
Keywords: Fat pad; Functional outcome; Gait analysis; Total knee arthroplasty.
© 2024. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- Hofstede SN, Gademan MGJ, Stijnen T, Nelissen RGHH, Marang-van de Mheen PJ (2018) group A-Os The influence of preoperative determinants on quality of life, functioning and pain after total knee and hip replacement: a pooled analysis of Dutch cohorts. BMC Musculoskelet Disord, 19(1):68–68 - PMC - PubMed
-
- Rathore S, Vadlamudi N, Lvsnr Y, Kumar AHA, Reddy IV, Krishnaiah K (2018) Fat pad excision in total knee arthroplasty does not affect functional outcome or anterior knee pain at 1year follow-up. J Arthrosc Joint Surg 5(1):29–32
-
- Clockaerts S, Bastiaansen-Jenniskens YM, Runhaar J et al (2010) The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: a narrative review. Osteoarthritis Cartilage 18(7):876–882 - PubMed
-
- Maculé F, Sastre S, Lasurt S, Sala P, Segur JM, Mallofré C (2005) Hoffa’s fat pad resection in total knee arthroplasty. Acta Orthop Belg 71(6):714–717 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
