

A novel positive end-expiratory pressure titration using electrical impedance tomography in spontaneously breathing acute respiratory distress syndrome patients on mechanical ventilation: an observational study from the MaastrICCht cohort
- PMID: 39196479
- PMCID: PMC11821668
- DOI: 10.1007/s10877-024-01212-8
A novel positive end-expiratory pressure titration using electrical impedance tomography in spontaneously breathing acute respiratory distress syndrome patients on mechanical ventilation: an observational study from the MaastrICCht cohort
Abstract
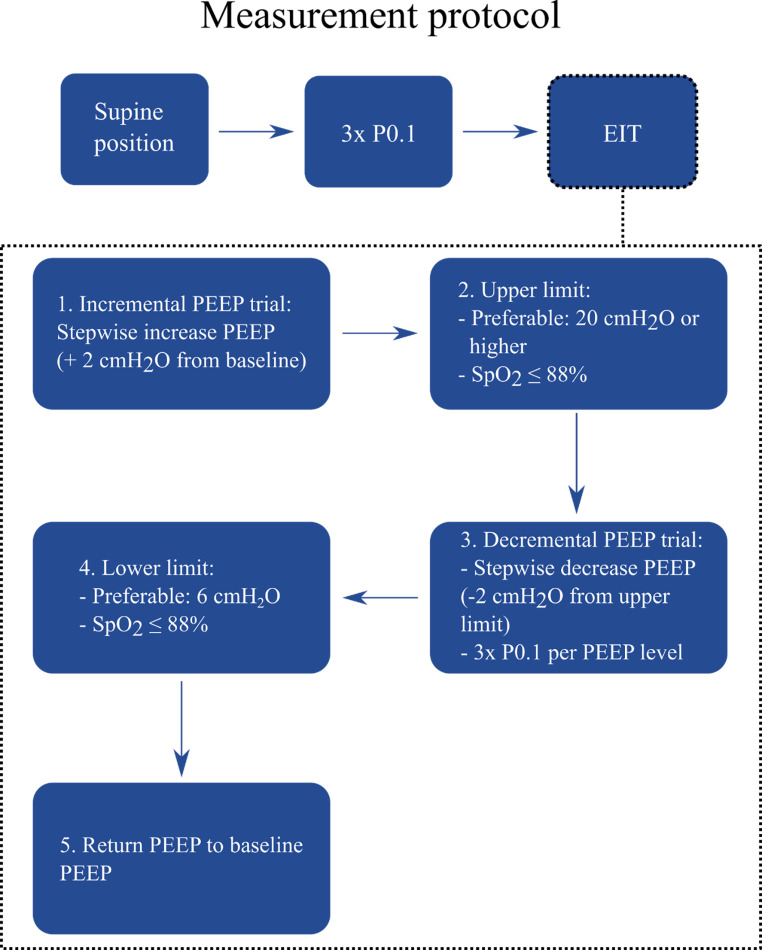
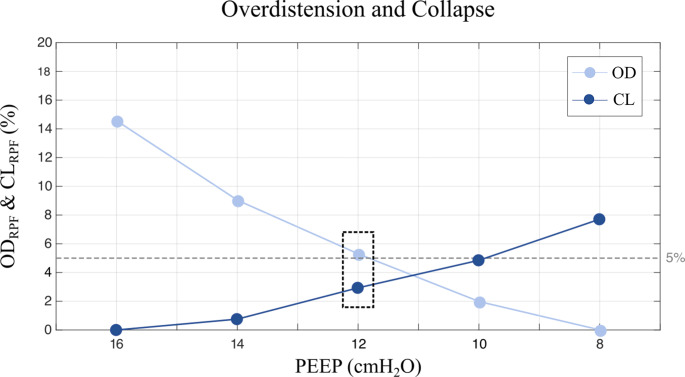
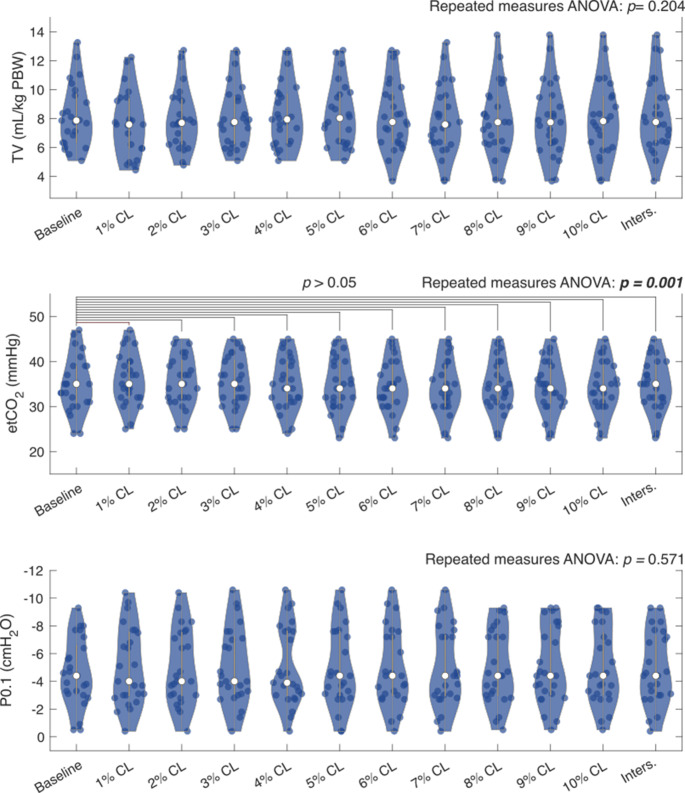
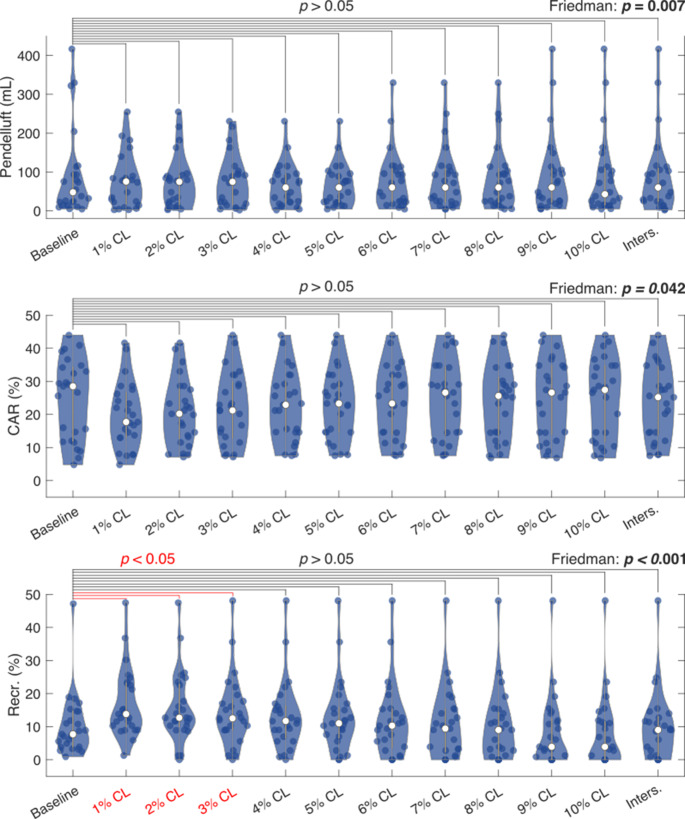
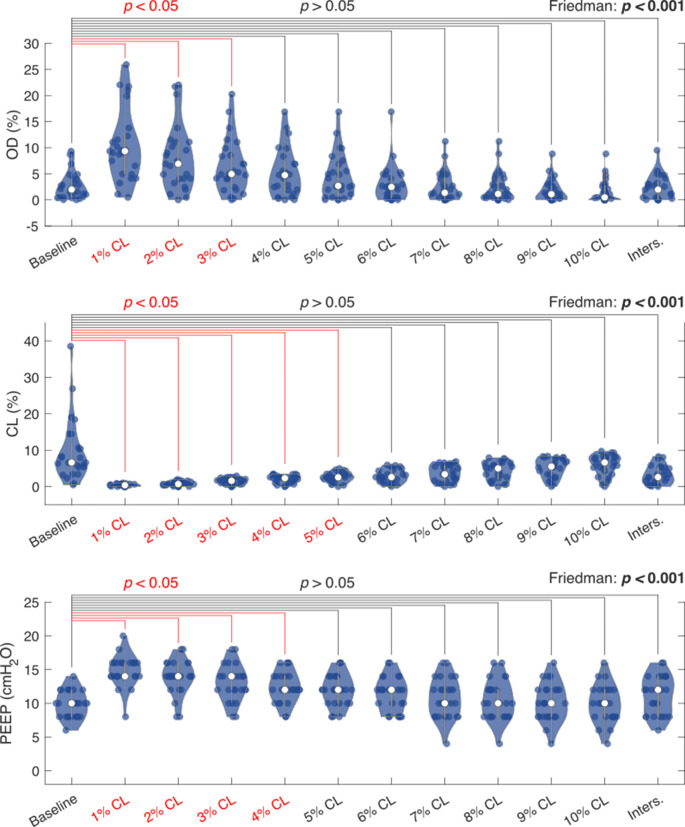
There is no universally accepted method for positive end expiratory pressure (PEEP) titration approach for patients on spontaneous mechanical ventilation (SMV). Electrical impedance tomography (EIT) guided PEEP-titration has shown promising results in controlled mechanical ventilation (CMV), current implemented algorithm for PEEP titration (based on regional compliance measurements) is not applicable in SMV. Regional peak flow (RPF, defined as the highest inspiratory flow rate based on EIT at a certain PEEP level) is a new method for quantifying regional lung mechanics designed for SMV. The objective is to study whether RPF by EIT is a feasible method for PEEP titration during SMV. Single EIT measurements were performed in COVID-19 ARDS patients on SMV. Clinical (i.e., tidal volume, airway occlusion pressure, end-tidal CO2) and mechanical (cyclic alveolar recruitment, recruitment, cumulative overdistension (OD), cumulative collapse (CL), pendelluft, and PEEP) outcomes were determined by EIT at several pre-defined PEEP thresholds (1-10% CL and the intersection of the OD and CL curves) and outcomes at all thresholds were compared to the outcomes at baseline PEEP. In total, 25 patients were included. No significant and clinically relevant differences were found between thresholds for tidal volume, end-tidal CO2, and P0.1 compared to baseline PEEP; cyclic alveolar recruitment rates changed by -3.9% to -37.9% across thresholds; recruitment rates ranged from - 49.4% to + 79.2%; cumulative overdistension changed from - 75.9% to + 373.4% across thresholds; cumulative collapse changed from 0% to -94.3%; PEEP levels from 10 up to 14 cmH2O were observed across thresholds compared to baseline PEEP of 10 cmH2O. A threshold of approximately 5% cumulative collapse yields the optimum compromise between all clinical and mechanical outcomes. EIT-guided PEEP titration by the RPF approach is feasible and is linked to improved overall lung mechanics) during SMV using a threshold of approximately 5% CL. However, the long-term clinical safety and effect of this approach remain to be determined.
Keywords: ARDS; Airway occlusion pressure; Electrical impedance tomography; Pendelluft; Positive end-expiratory pressure; Regional peak flow; Spontaneous ventilation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study is approved by the ethical committee of the Maastricht University Medical Center + and University of Maastricht (METC: 2020 − 1565), registered in NTR with number NL8613, and conducted in accordance with the Declaration of Helsinki (as revised in 2013). During the pandemic, the board of directors of the Maastricht UMC + adopted a policy to inform patients or their legal representative and ask for their consent to use their data for COVID-19 research purposes. Consent for publication: Not applicable. Competing interests: SH, SdJ, DB have a patent on the algorithm (International Publication Number: WO 2024/003413 A1) used in the present manuscript to quantify regional and cumulative overdistension and collapse. The remaining authors do not have any other competing interests related to this study.
Figures
References
-
- Guldner A, Kiss T, Bluth T, Uhlig C, Braune A, Carvalho N, et al. Effects of ultraprotective ventilation, extracorporeal carbon dioxide removal, and spontaneous breathing on lung morphofunction and inflammation in experimental severe acute respiratory distress syndrome. Anesthesiology. 2015;122(3):631–46. - PubMed
-
- Yoshida T, Torsani V, Gomes S, De Santis RR, Beraldo MA, Costa EL, et al. Spontaneous effort causes occult pendelluft during mechanical ventilation. Am J Respir Crit Care Med. 2013;188(12):1420–7. - PubMed
-
- Yoshida T, Uchiyama A, Matsuura N, Mashimo T, Fujino Y. Spontaneous breathing during lung-protective ventilation in an experimental acute lung injury model: high transpulmonary pressure associated with strong spontaneous breathing effort may worsen lung injury. Crit Care Med. 2012;40(5):1578–85. - PubMed
-
- Yoshida T, Uchiyama A, Matsuura N, Mashimo T, Fujino Y. The comparison of spontaneous breathing and muscle paralysis in two different severities of experimental lung injury. Crit Care Med. 2013;41(2):536–45. - PubMed
-
- Mauri T, Langer T, Zanella A, Grasselli G, Pesenti A. Extremely high transpulmonary pressure in a spontaneously breathing patient with early severe ARDS on ECMO. Intensive Care Med. 2016;42(12):2101–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
