

Body Mass Index and Risk of Colorectal Cancer Incidence and Mortality in Asia
- PMID: 39196559
- PMCID: PMC11358861
- DOI: 10.1001/jamanetworkopen.2024.29494
Body Mass Index and Risk of Colorectal Cancer Incidence and Mortality in Asia
Abstract
Importance: The global burden of obesity is increasing, as are colorectal cancer (CRC) incidence and mortality.
Objectives: To assess the association between body mass index (BMI) and risks of incident CRC and CRC-related death in the Asian population.
Design, setting, and participants: This cohort study includes data pooled from 17 prospective cohort studies included in The Asia Cohort Consortium. Cohort enrollment was conducted from January 1, 1984, to December 31, 2002. Median follow-up time was 15.2 years (IQR, 12.1-19.2 years). Data were analyzed from January 15, 2023, through January 15, 2024.
Exposure: Body mass index, calculated as weight in kilograms divided by height in meters squared.
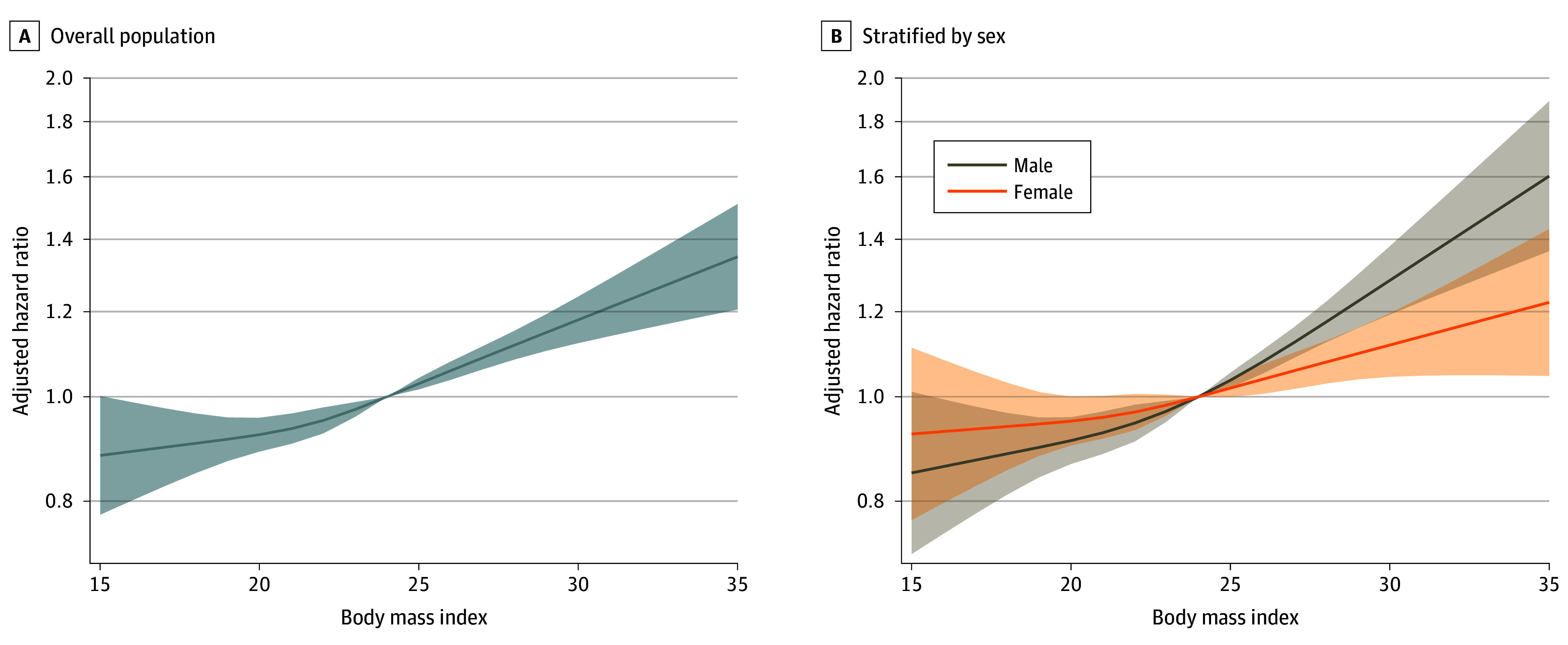
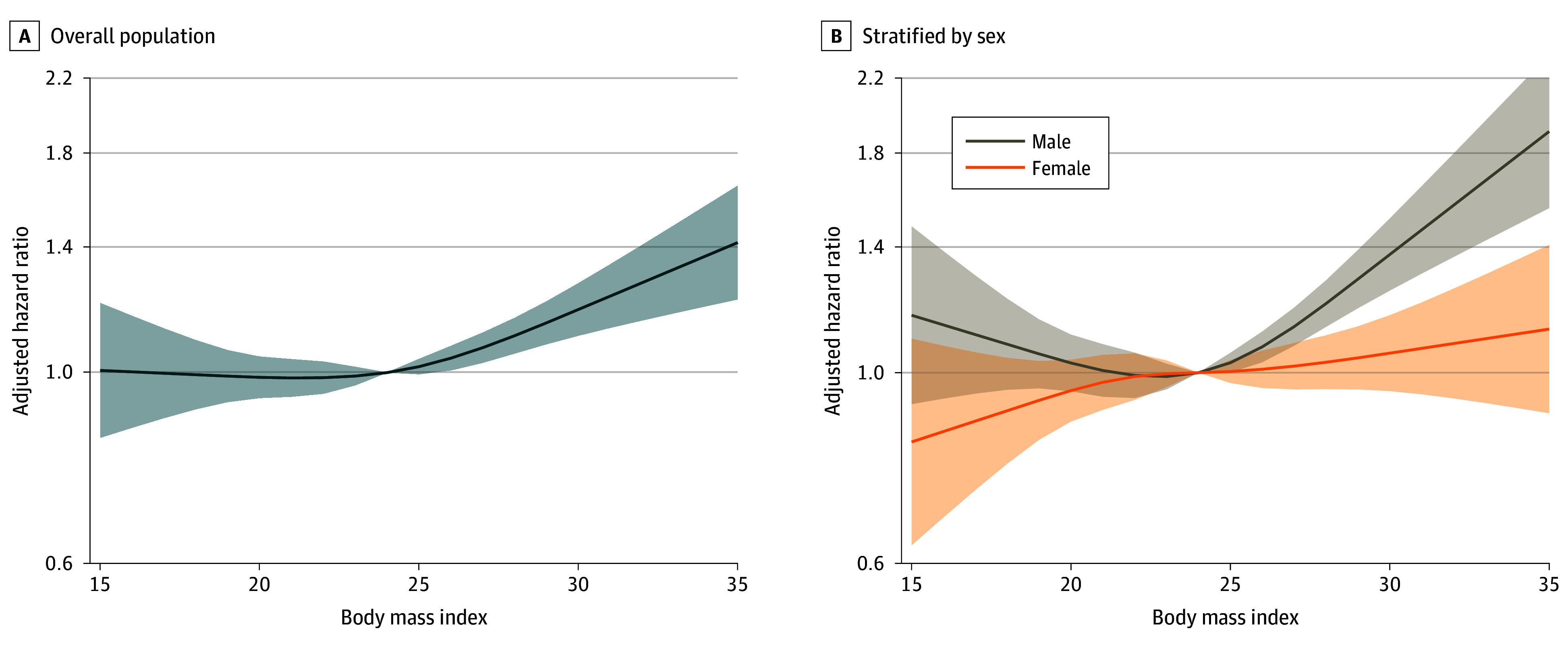
Main outcomes and measures: The primary outcomes were CRC incidence and CRC-related mortality. The risk of events is reported as adjusted hazard ratios (AHRs) and 95% CIs for incident CRC and death from CRC using the Cox proportional hazards regression model.
Results: To assess the risk of incident CRC, 619 981 participants (mean [SD] age, 53.8 [10.1] years; 52.0% female; 11 900 diagnosed incident CRC cases) were included in the study, and to assess CRC-related mortality, 650 195 participants (mean [SD] age, 53.5 [10.2] years; 51.9% female; 4550 identified CRC deaths) were included in the study. A positive association between BMI and risk of CRC was observed among participants with a BMI greater than 25.0 to 27.5 (AHR, 1.09 [95% CI, 1.03-1.16]), greater than 27.5 to 30.0 (AHR, 1.19 [95% CI, 1.11-1.29]), and greater than 30.0 (AHR, 1.32 [95% CI, 1.19-1.46]) compared with those with a BMI greater than 23.0 to 25.0 (P < .001 for trend), and BMI was associated with a greater increase in risk for colon cancer than for rectal cancer. A similar association between BMI and CRC-related death risk was observed among participants with a BMI greater than 27.5 (BMI >27.5-30.0: AHR, 1.18 [95% CI, 1.04-1.34]; BMI >30.0: AHR, 1.38 [95% CI, 1.18-1.62]; P < .001 for trend) and was present among men with a BMI greater than 30.0 (AHR, 1.87 [95% CI, 1.49-2.34]; P < .001 for trend) but not among women (P = .15 for trend) (P = .02 for heterogeneity).
Conclusions and relevance: In this cohort study that included a pooled analysis of 17 cohort studies comprising participants across Asia, a positive association between BMI and CRC incidence and related mortality was found. The risk was greater among men and participants with colon cancer. These findings may have implications to better understand the burden of obesity on CRC incidence and related deaths in the Asian population.
Conflict of interest statement
Figures
References
-
- GBD 2019 Colorectal Cancer Collaborators . Global, regional, and national burden of colorectal cancer and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol. 2022;7(7):627-647. doi: 10.1016/S2468-1253(22)00044-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
