

Quantifying extent of meningioma preoperative embolization through volumetric analysis: A retrospective case series
- PMID: 39197867
- PMCID: PMC11569758
- DOI: 10.1177/15910199241267312
Quantifying extent of meningioma preoperative embolization through volumetric analysis: A retrospective case series
Abstract
Background: Endovascular embolization is an adjunct to meningioma resection. Isolating the effectiveness of embolization is difficult as MR imaging is typically performed before embolization and after resection, and volumetric assessment of embolization on 2D angiographic imaging is challenging. We investigated the correlation between 2D angiographic and 3D MR measurements of meningioma devascularization following embolization.
Methods: We implemented a protocol for postembolization, preresection MRI. Angiographic devascularization was graded according to reduction of tumor blush from 1 (partial embolization) to 4 (complete embolization with no residual circulation supply). Volumetric extent of embolization was quantified as the percent of tumor contrast enhancement lost following embolization. Tumor embolization was analyzed according to tumor location and vascular supply.
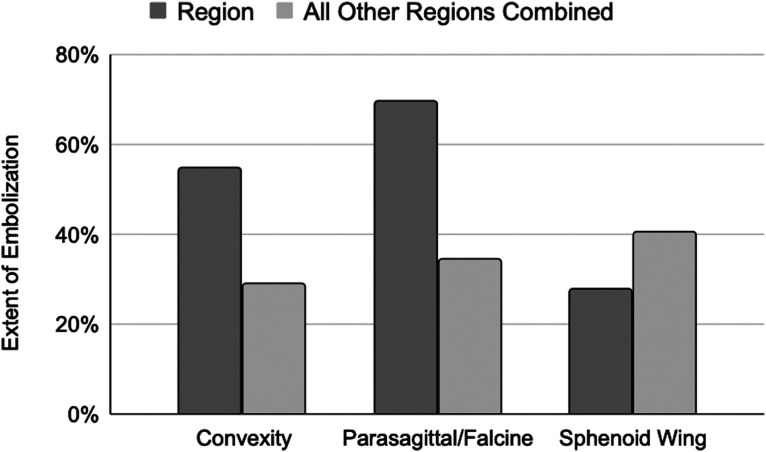
Results: Thirty consecutive patients met inclusionary criteria. Grade 1 devascularization was achieved in 7% of patients, grade 2 in 43%, grade 3 in 20%, and grade 4 in 30%. Average extent of embolization was 37 ± 6%. Extent of tumor embolization was low (<25%) in 40%, moderate (25%-75%) in 40%, and high (>75%) in 20% of patients. Convexity, parasagittal/falcine and sphenoid wing tumors were found to have distinct vascular supply patterns and extent of embolization. Angiographic devascularization grade was significantly correlated with volumetric extent of tumor embolization (p < 0.001, r = 0.758).
Conclusion: This is the first study to implement postembolization, preoperative MRI to assess extent of embolization prior to meningioma resection. The study demonstrates that volumetric assessment of contrast reduction following embolization provides a quantitative and spatially resolved framework for assessing extent of tumor embolization.
Keywords: Tumor embolization; image segmentation; meningioma; volumetric analysis.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



References
-
- Gruber P, Schwyzer L, Klinger E, et al. Longitudinal imaging of tumor volume, diffusivity, and perfusion after preoperative endovascular embolization in supratentorial hemispheric meningiomas. World Neurosurg 2018; 120: e357–e364. - PubMed
-
- Schartz D, Manganaro M, Szekeres D, et al. Direct percutaneous puncture versus transarterial embolization for head and neck paragangliomas: a systematic review and meta-analysis. Interv Neuroradiol 2023; 29: 15910199231188859. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
