

Gut Microbiome Wellness Index 2 enhances health status prediction from gut microbiome taxonomic profiles
- PMID: 39198444
- PMCID: PMC11358288
- DOI: 10.1038/s41467-024-51651-9
Gut Microbiome Wellness Index 2 enhances health status prediction from gut microbiome taxonomic profiles
Abstract
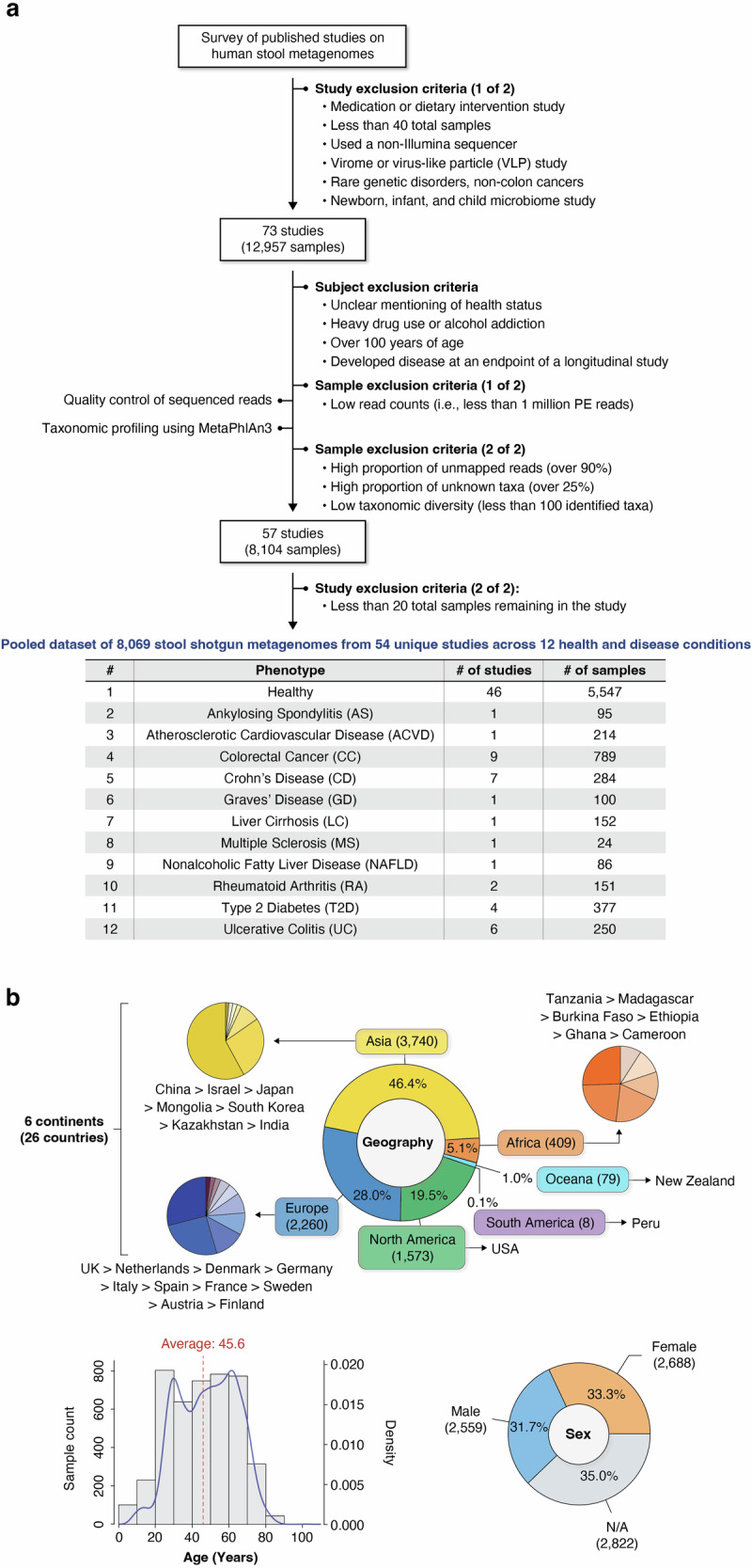
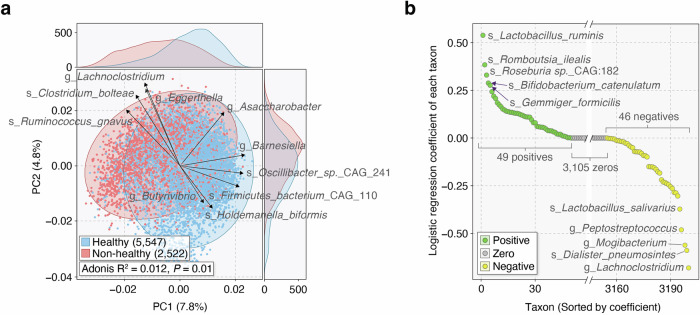
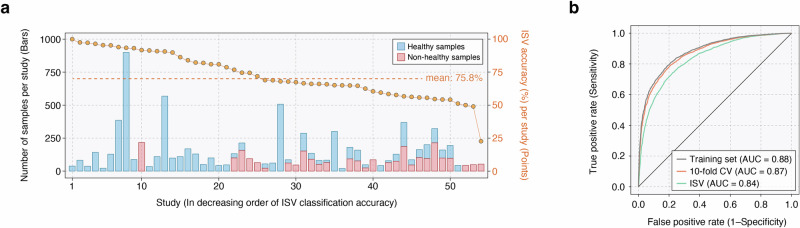
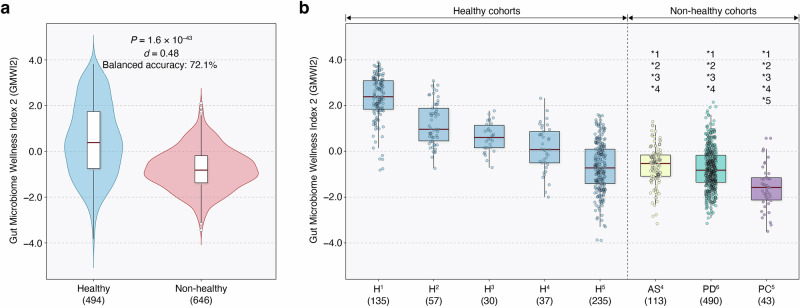
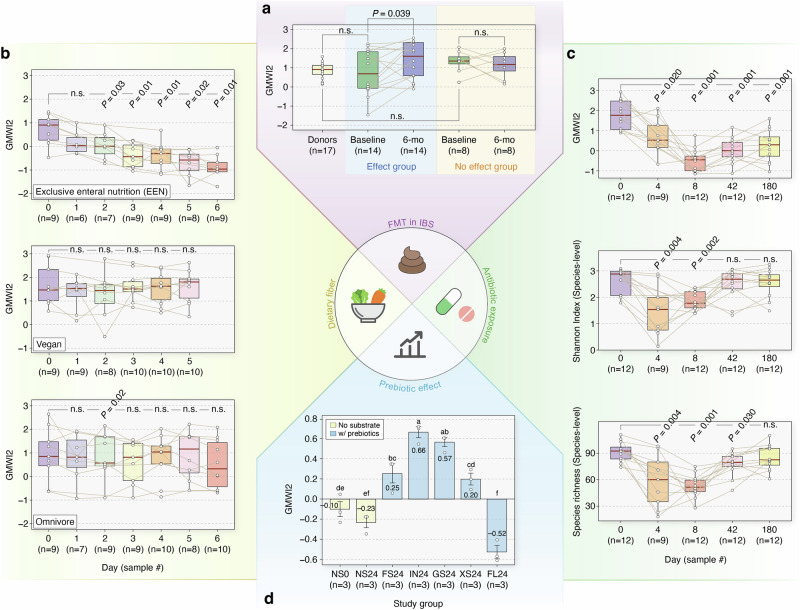
Recent advancements in translational gut microbiome research have revealed its crucial role in shaping predictive healthcare applications. Herein, we introduce the Gut Microbiome Wellness Index 2 (GMWI2), an enhanced version of our original GMWI prototype, designed as a standardized disease-agnostic health status indicator based on gut microbiome taxonomic profiles. Our analysis involves pooling existing 8069 stool shotgun metagenomes from 54 published studies across a global demographic landscape (spanning 26 countries and six continents) to identify gut taxonomic signals linked to disease presence or absence. GMWI2 achieves a cross-validation balanced accuracy of 80% in distinguishing healthy (no disease) from non-healthy (diseased) individuals and surpasses 90% accuracy for samples with higher confidence (i.e., outside the "reject option"). This performance exceeds that of the original GMWI model and traditional species-level α-diversity indices, indicating a more robust gut microbiome signature for differentiating between healthy and non-healthy phenotypes across multiple diseases. When assessed through inter-study validation and external validation cohorts, GMWI2 maintains an average accuracy of nearly 75%. Furthermore, by reevaluating previously published datasets, GMWI2 offers new insights into the effects of diet, antibiotic exposure, and fecal microbiota transplantation on gut health. Available as an open-source command-line tool, GMWI2 represents a timely, pivotal resource for evaluating health using an individual's unique gut microbial composition.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Update of
-
Gut Microbiome Wellness Index 2 for Enhanced Health Status Prediction from Gut Microbiome Taxonomic Profiles.bioRxiv [Preprint]. 2023 Oct 2:2023.09.30.560294. doi: 10.1101/2023.09.30.560294. bioRxiv. 2023. Update in: Nat Commun. 2024 Aug 28;15(1):7447. doi: 10.1038/s41467-024-51651-9. PMID: 37873265 Free PMC article. Updated. Preprint.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
