

Patient resuscitated after cardiopulmonary arrest exhibits abnormally increased phenytoin metabolic rate due to unknown factors: a case report
- PMID: 39198905
- PMCID: PMC11360309
- DOI: 10.1186/s40780-024-00374-6
Patient resuscitated after cardiopulmonary arrest exhibits abnormally increased phenytoin metabolic rate due to unknown factors: a case report
Abstract
Background: Fosphenytoin (FOS) is a prodrug of phenytoin (PHT) with a metabolism that exhibits Michaelis-Menten-type kinetics. Genetic polymorphisms of the metabolic enzymes of PHT make it challenging to predict its plasma concentrations. High plasma PHT concentrations are typically problematic, and several causes have been elucidated. In contrast, cases of patients with low PHT plasma concentrations that did not increase despite the administration of appropriate PHT doses have been reported, and the causes may include changes in plasma protein-binding rates, genetic mutations, and concomitant use of drugs that induce liver enzymes; however, even these factors do not explain the low PHT plasma concentrations in some cases.
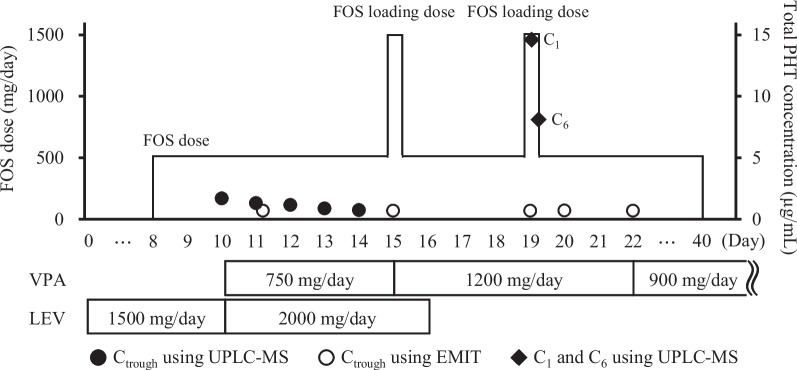
Case presentation: We encountered the case of a patient with plasma PHT concentrations that were continuously < 0.7 µg/mL after daily use of FOS for seizures that occurred after cardiopulmonary arrest. We analyzed the protein-unbound fraction, urinary metabolites, and related genes to investigate the cause. False negatives due to the measurement method, errors in dosage and administration method, and increased excretion of PHT were excluded. Hepatic metabolic activity of PHT increased to 4.6-6.1 times the normal level. The S/R ratio of 5-(p-hydroxyphenyl)-5-phenylhydantoin-glucuronide, a major PHT metabolite, was normal at 15.2, suggesting increased activities of CYP2C9 and CYP2C19. Furthermore, the protein-unbound fraction of PHT was 5.2-6.9%, CYP2C19*17 was wild type, and there was no concomitant drug use to induce both enzymes.
Conclusions: The low PHT plasma concentration in this patient was found to be caused by increased hepatic metabolic activity that could not be explained by known factors. Careful monitoring is necessary to consider the possibility of increased hepatic metabolic activity in similar cases.
Keywords: Cardiopulmonary arrest; Fosphenytoin; Pharmacokinetics; Phenytoin; Therapeutic drug monitoring.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gerber N, Mays DC, Donn KH, Laddu A, Guthrie RM, Turlapaty P, et al. Safety, tolerance and pharmacokinetics of intravenous doses of the phosphate ester of 3-hydroxymethyl-5,5-diphenylhydantoin: a new prodrug of phenytoin. J Clin Pharmacol. 1988;28:1023–32. 10.1002/j.1552-4604.1988.tb03124.x - DOI - PubMed
-
- Patsalos PN, Berry DJ, Bourgeois BF, Cloyd JC, Glauser TA, Johannessen SI, et al. Antiepileptic drugs—best practice guidelines for therapeutic drug monitoring: a position paper by the subcommission on therapeutic drug monitoring. ILAE Commission on Therapeutic Strategies Epilepsia. 2008;49:1239–76. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
