

Expanding the genetic landscape of Usher syndrome type IV caused by pathogenic ARSG variants
- PMID: 39199020
- PMCID: PMC11608847
- DOI: 10.1111/cge.14614
Expanding the genetic landscape of Usher syndrome type IV caused by pathogenic ARSG variants
Abstract
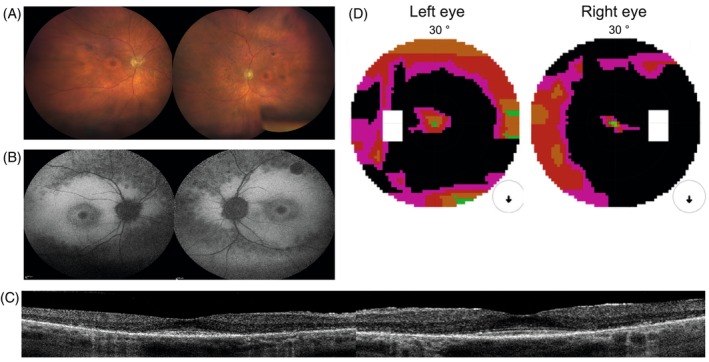
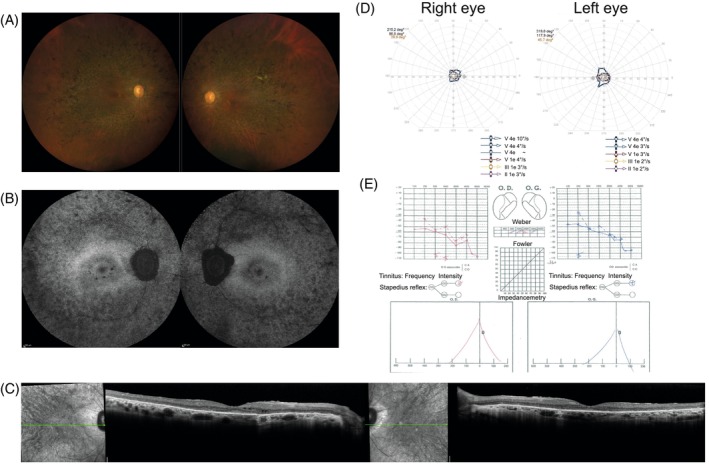
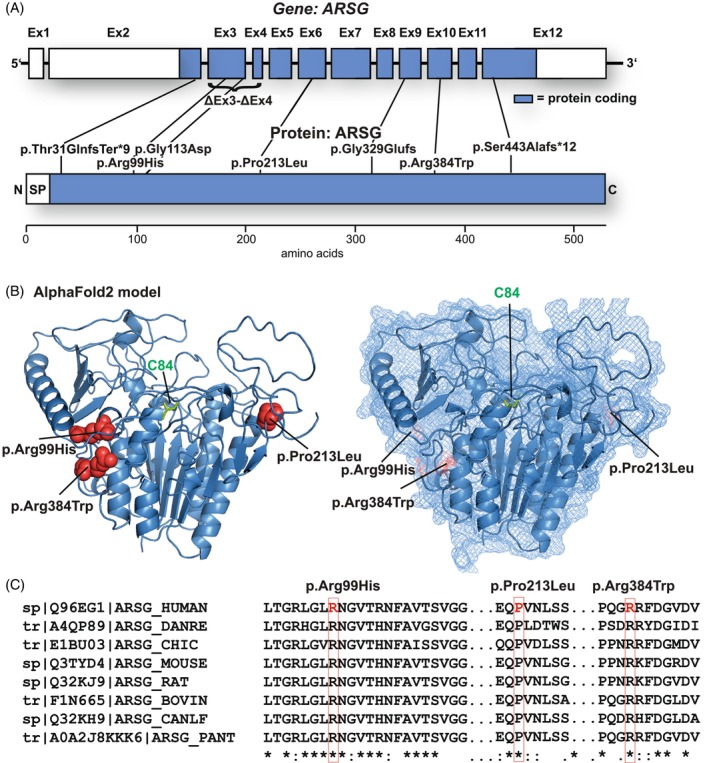
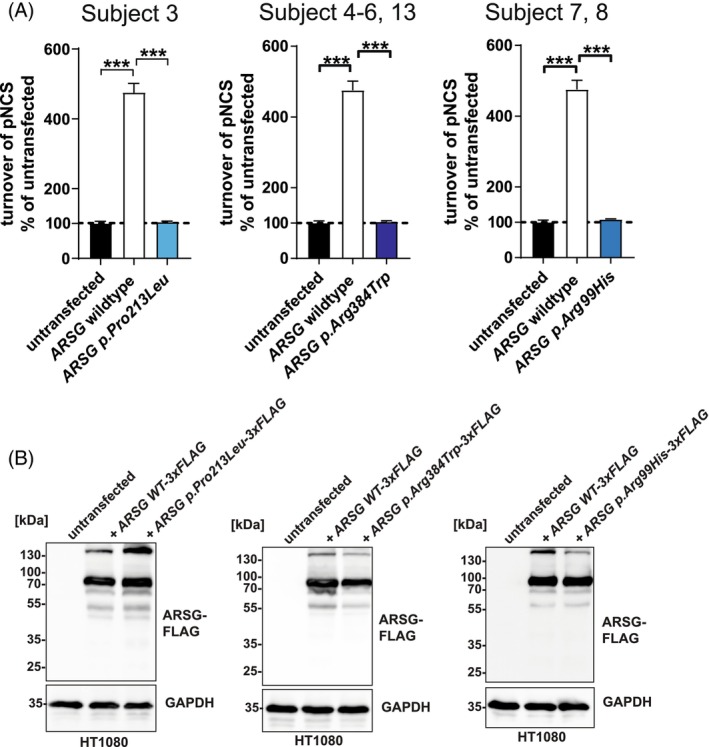
Usher syndrome (USH) is the most common cause of deafblindness. USH is autosomal recessively inherited and characterized by rod-cone dystrophy or retinitis pigmentosa (RP), often accompanied by sensorineural hearing loss. Variants in >15 genes have been identified as causative for clinically and genetically distinct subtypes. Among the ultra-rare and recently discovered genes is ARSG, coding for the lysosomal sulfatase Arylsulfatase G. This subtype was assigned as "USH IV" with a late onset of RP and usually late-onset progressive SNHL without vestibular involvement. Here, we describe nine new subjects and the clinical description of four cases with the USH IV phenotype bearing seven novel and two known pathogenic variants. Functional experiments indicated the complete loss of sulfatase enzymatic activity upon ectopic expression of mutated ARSG cDNA. Interestingly, we identified a homozygous missense variant, p.(Arg99His), previously described in dogs with neuronal ceroid lipofuscinosis. Our study expands the genetic landscape of ARSG-USH IV and the number of known subjects by more than 30%. These findings highlight that USH IV likely has been underdiagnosed and emphasize the need to test molecularly unresolved subjects with deafblindness syndrome. Finally, testing of ARSG should be considered for the genetic work-up of apparent isolated inherited retinal diseases.
Keywords: ARSG; Usher syndrome (USH); canine variant p.(Arg99His); lysosomal sulfatase; retinitis pigmentosa (RP); rod‐cone dystrophy (RCD); sensorineural hearing loss (SNHL).
© 2024 The Author(s). Clinical Genetics published by John Wiley & Sons Ltd.
Conflict of interest statement
None of the authors declares any competing interests or conflicts of interest.
Figures
References
-
- Khateb S, Kowalewski B, Bedoni N, et al. A homozygous founder missense variant in arylsulfatase G abolishes its enzymatic activity causing atypical Usher syndrome in humans. Genet Med. 2018;20(9):1004‐1012. - PubMed
-
- Kruszewski K, Lullmann‐Rauch R, Dierks T, Bartsch U, Damme M. Degeneration of photoreceptor cells in arylsulfatase G‐deficient mice. Invest Ophthalmol Vis Sci. 2016;57(3):1120‐1131. - PubMed
MeSH terms
Substances
Grants and funding
- Union Nationale des Aveugles et Déficients Visuels
- ZIA EY000564/ImNIH/Intramural NIH HHS/United States
- ANR-11-IDEX-0004-0/IHU FOReSIGHT
- ANR-18-IAHU-0001/Retina France
- BR-GE-0619-0761-INSERM/Foundation Fighting Blindness center
- FWO-1802220N/EJPRD19-234 Solve-RET
- ANR10-LABX-65/LABEX LIFESENSES
- Fondation Voir et Entendre
- ANR-18-IAHU-01/Retina France
- National Eye Institute, National Institutes of Health
- C-CMM-0907-0428-INSERM04/Foundation Fighting Blindness center
- UNADEV in partnership with ITMO NNP/AVIESAN
- BOF20/GOA/023/Universiteit Gent
LinkOut - more resources
Full Text Sources
Medical
