

Vertical Ex Vivo Dermoscopy in Assessment of Malignant Skin Lesions
- PMID: 39200148
- PMCID: PMC11351155
- DOI: 10.3390/biomedicines12081683
Vertical Ex Vivo Dermoscopy in Assessment of Malignant Skin Lesions
Abstract
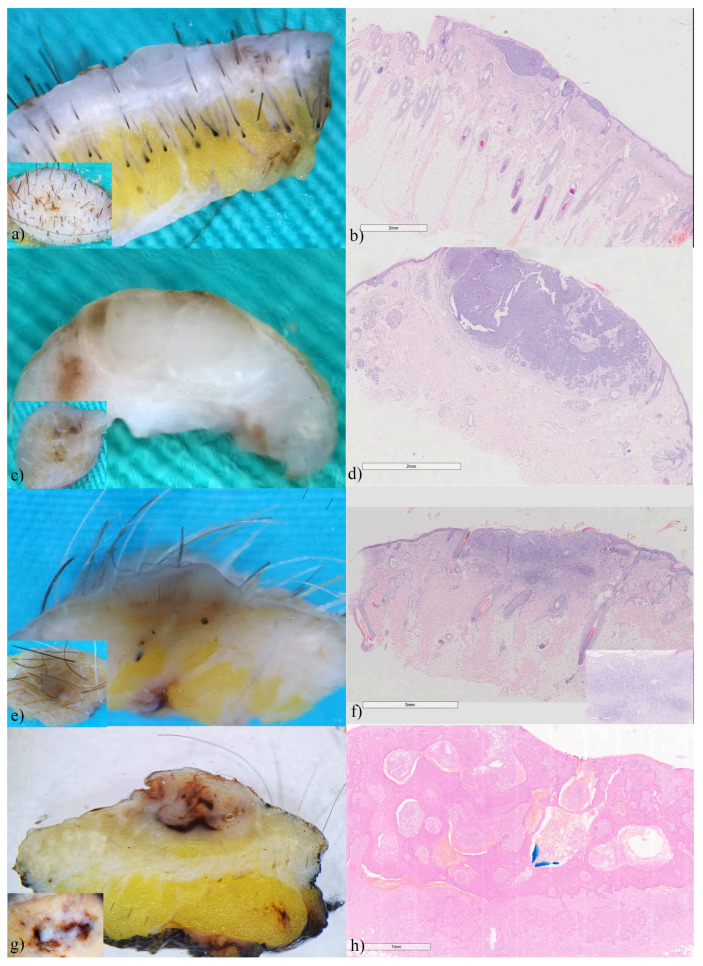
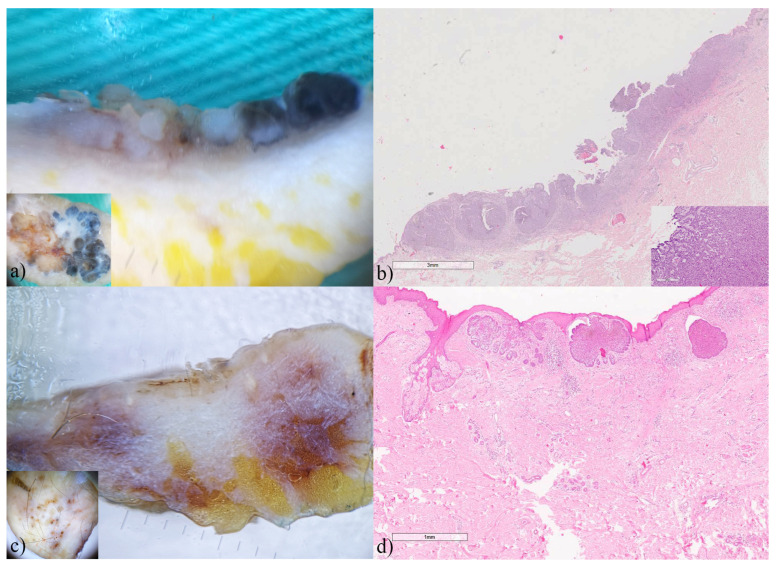
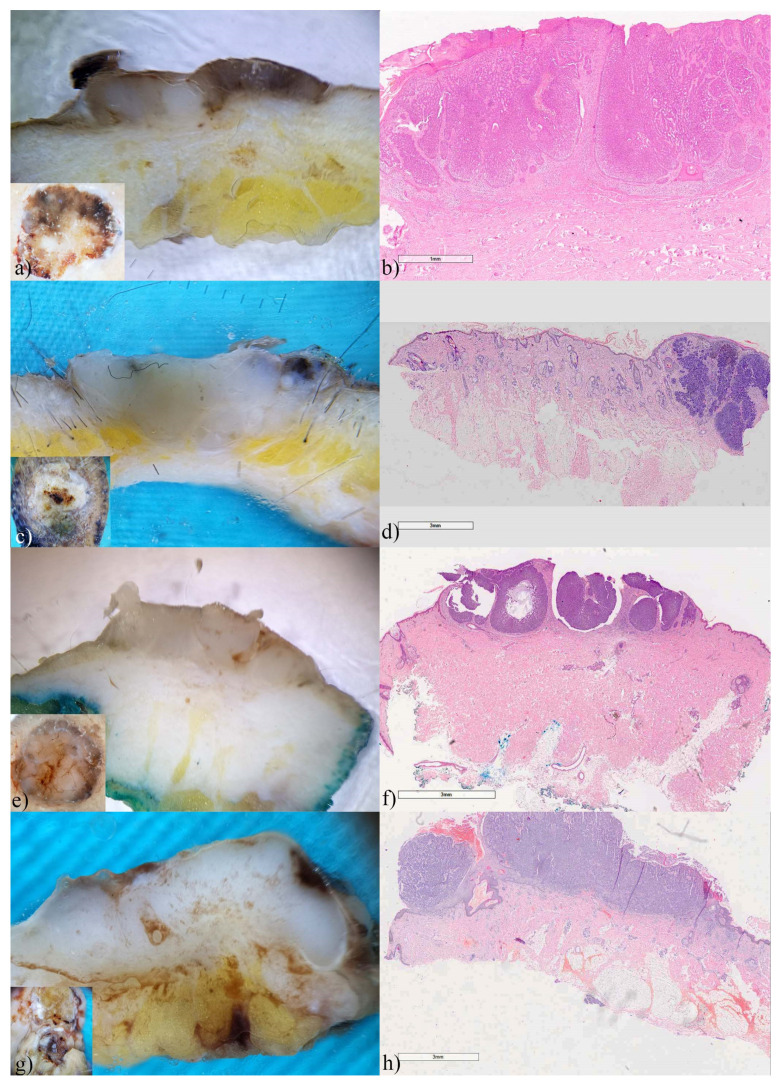
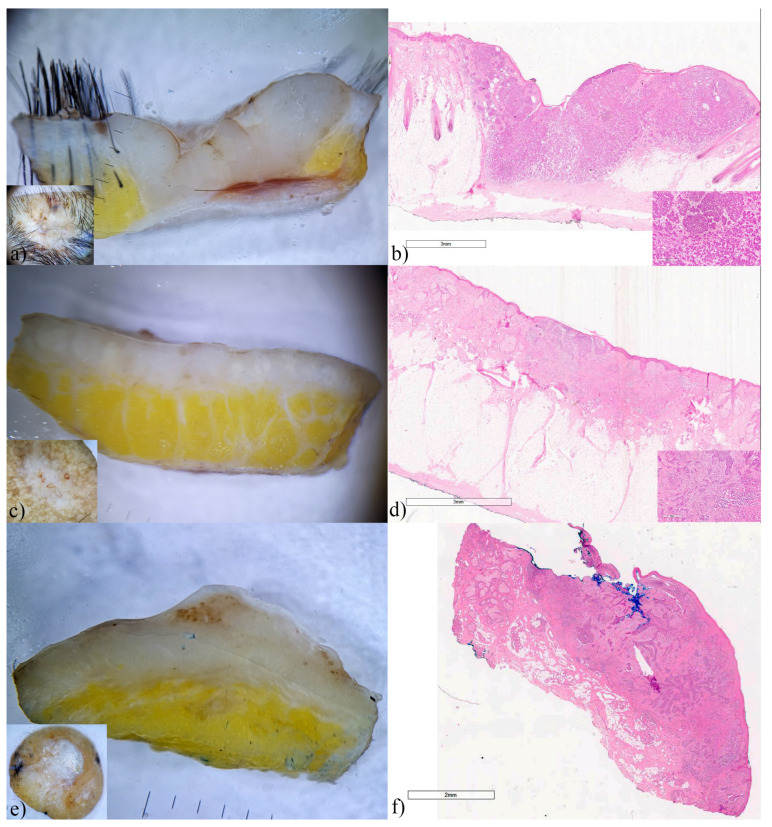
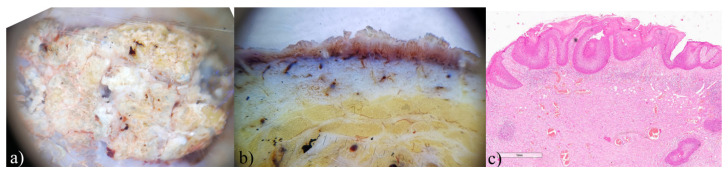
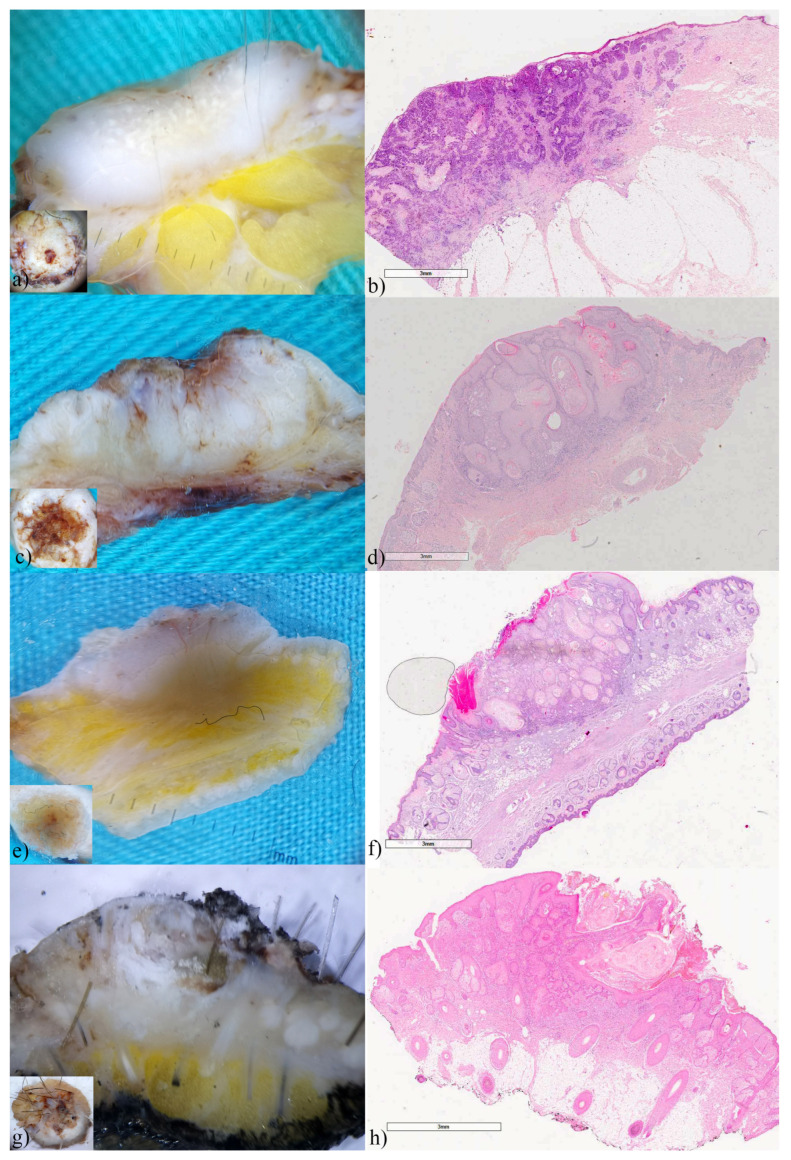
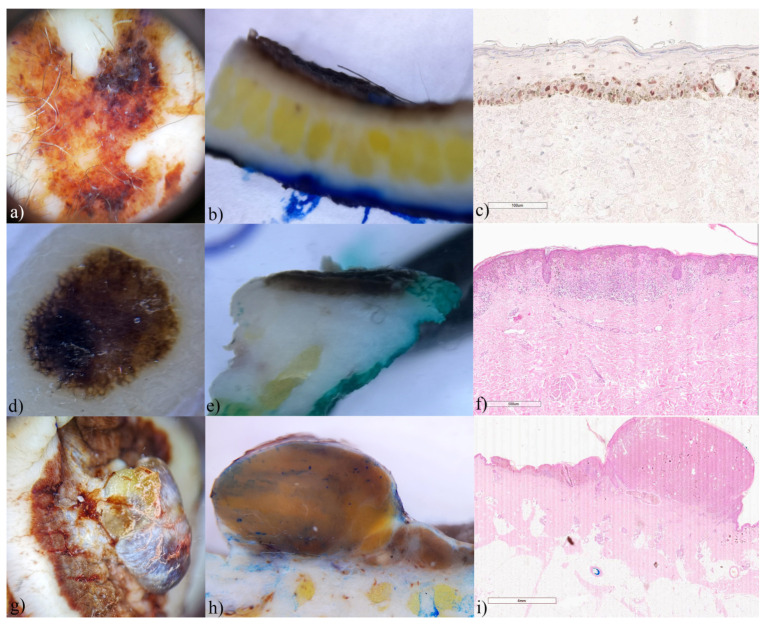
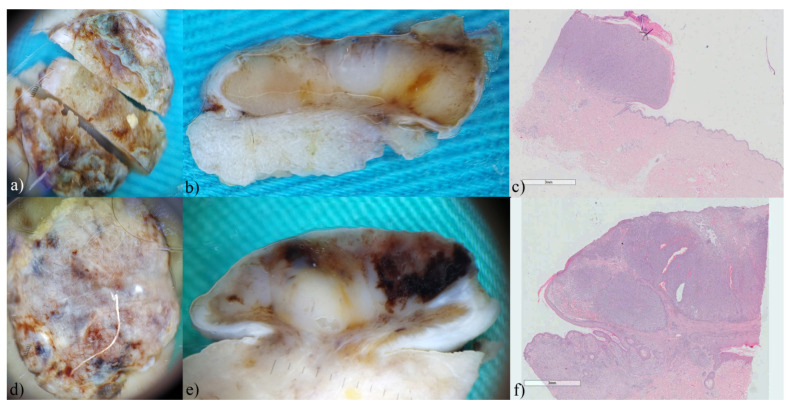
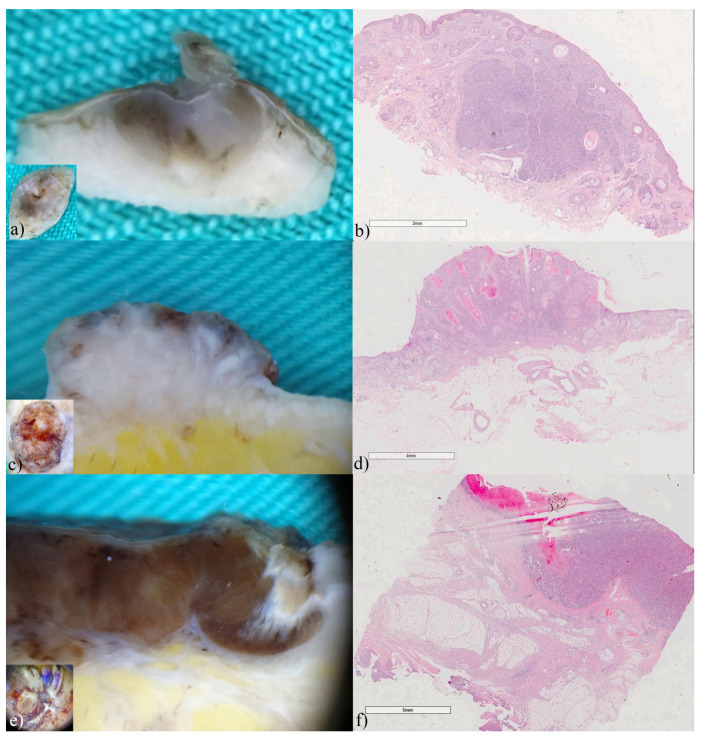
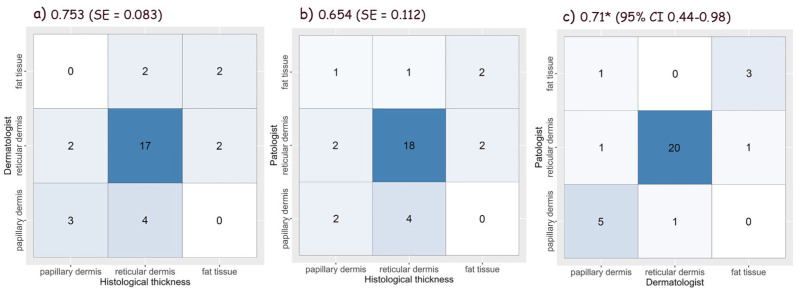
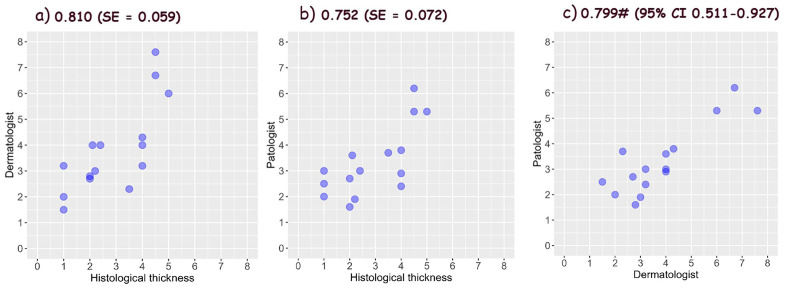
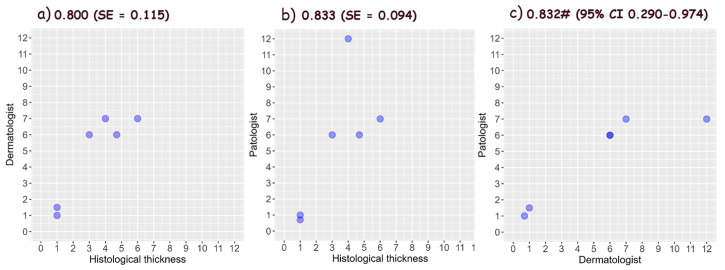
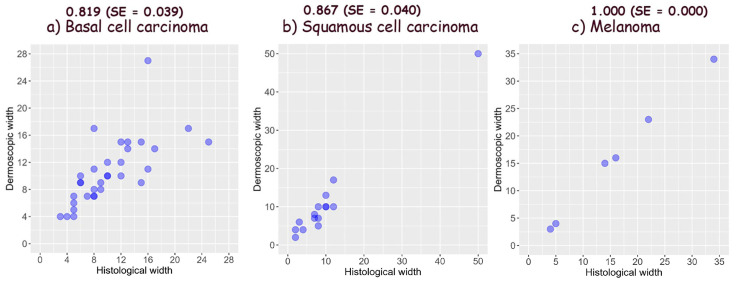
The role of vertical ex vivo dermoscopy relevant to clinical diagnosis has not been investigated yet. Study objectives were defining, describing, and determining the importance of the structures visible using vertical ex vivo dermoscopy in the diagnosis of malignant skin lesions, as well as determining their accuracy in the assessment of tumor margins. A prospective, descriptive study was conducted in two University centers. Digital images of completely excised skin lesions, fixed in formalin, before histopathological diagnosis were used for analysis. BCCs had the most diverse dermoscopic presentation on the vertical section, while SCCs showed a similar presentation in most cases. Vertical dermoscopy of thin melanomas was almost identical, unlike nodular melanomas. Thickness accuracy assessed by dermatologist was 0.753 for BCC, 0.810 for SCC, and 0.800 for melanomas, whereas assessment by pathologist was 0.654, 0.752, and 0.833, respectively. The accuracy of tumor width assessment was 0.819 for BCCs, 0.867 for SCCs and 1.000 for melanoma as estimated by a Dermatologist. Interobserver agreement was 0.71 for BCC, 0.799 for SCC and 0.832 for melanomas. Vertical ex vivo dermoscopy may contribute to the distinction between BCCs, SCCs, and melanomas. Moreover, regardless of the doctor's specialty, it enables a good assessment of the tumor's margins.
Keywords: dermoscopy; ex vivo; histopathology; malignant skin lesions; vertical view.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
