

Biologics in T2 Severe Asthma: Unveiling Different Effectiveness by Real-World Indirect Comparison
- PMID: 39200892
- PMCID: PMC11355661
- DOI: 10.3390/jcm13164750
Biologics in T2 Severe Asthma: Unveiling Different Effectiveness by Real-World Indirect Comparison
Abstract
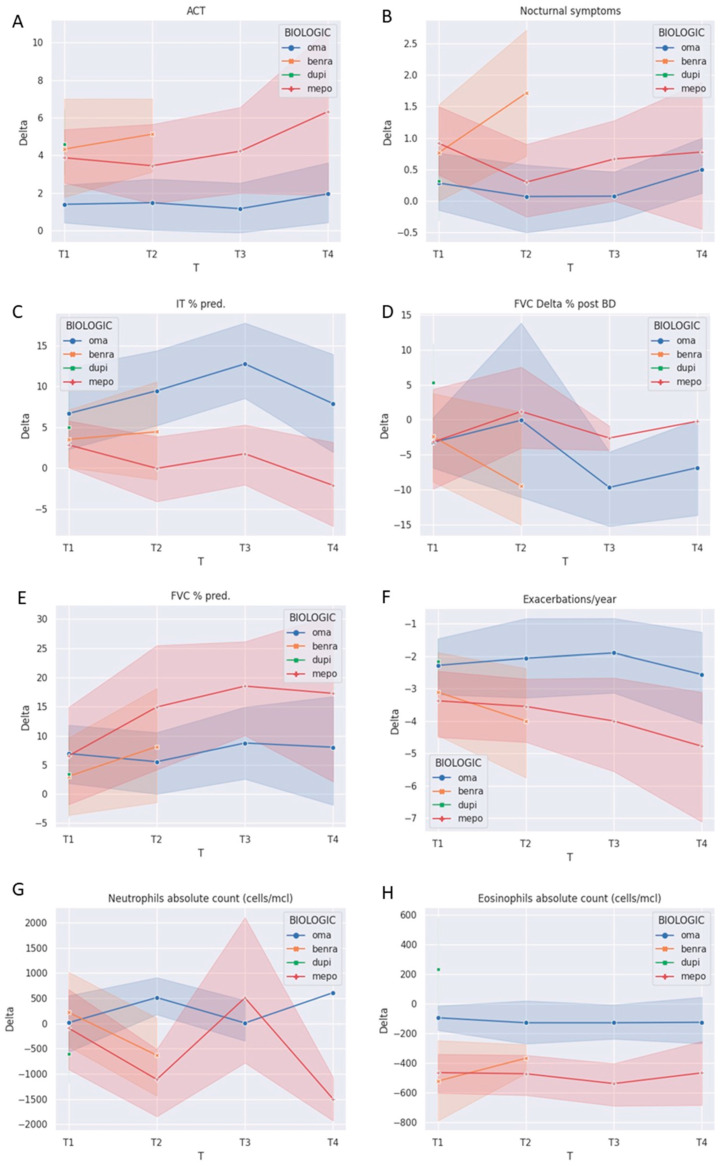
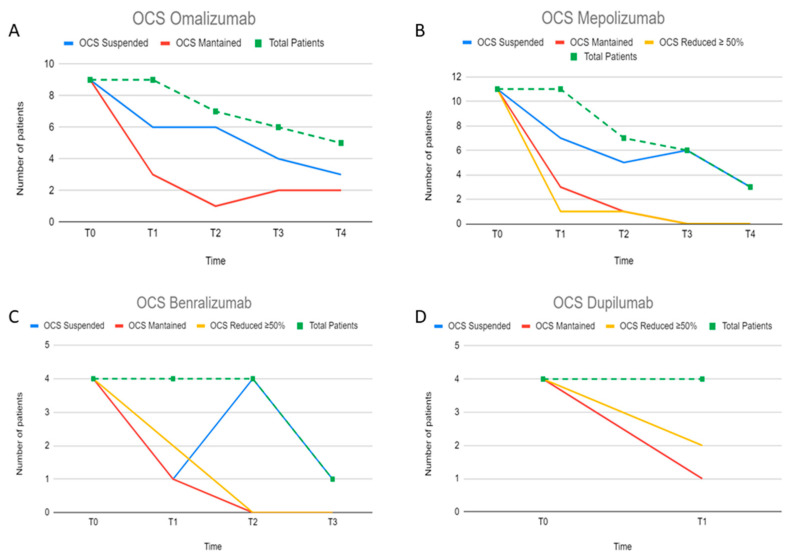
Background: Indirect comparison among biologics in severe asthma (SA) is a challenging but desirable goal for clinicians in real life. The aim of the study is to define characteristics of a biologic-treated T2-driven-SA population and to evaluate the effectiveness of biologic treatments in a real-world setting by variation in intra/inter-biologic parameters in an up to 4-year follow-up. Methods: Demographic, clinical, functional, and biological characteristics were evaluated retrospectively in 104 patients recruited until July 2022 at baseline (T0) and over a maximum of 4 years (T4) of biologic therapy (omalizumab/OmaG = 41, from T0 to T4, mepolizumab/MepoG = 26, from T0 to T4, benralizumab/BenraG = 18, from T0 to T2, and dupilumab/DupiG = 19, from T0 to T1). Variations of parameters using means of paired Delta were assessed. Results: At baseline, patients had high prevalence of T2-driven comorbidities, low asthma control test (ACT mean 17.65 ± 4.41), impaired pulmonary function (FEV1 65 ± 18 %pred), frequent exacerbations/year (AEs 3.5 ± 3), and OCS dependence (60%). DupiG had lower T2 biomarkers/comorbidities and AEs, and worse FEV1 (57 ± 19 %pred) compared to other biologics (p < 0.05). All biologics improved ACT, FEV1%, FVC%, AEs rate, and OCS use. FEV1% improved in MepoG and BenraG over the minimal clinically important difference and was sustained over 4 years in OmaG and MepoG. A significant RV reduction in OmaG (T4) and DupiG (T1), and BenraG normalization (T2) of airflow limitation were found. We observed through inter-biologic parameters pair delta variation comparison a significant nocturnal awakenings reduction in BenraG vs. OmaG/MepoG, and neutrophils reduction in BenraG/DupiG vs. OmaG. Conclusions: Indirect comparison among biologics unveils clinical and functional improvements that may mark a different effectiveness. These results may highlight the preference of a single biologic compared to another with regard to specific treatable traits.
Keywords: benralizumab; biologics; dupilumab; indirect comparison; mepolizumab; omalizumab; precision medicine; severe asthma; treatable traits.
Conflict of interest statement
G.G. reports fee as speaker for AstraZeneca; F.L.M.R. reports grants, personal fees, and other compensation from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, and Novartis, and personal fees and grants to support scientific research from Sanofi, all outside of the submitted work. M.B. is an employer of Re Learn S.R.L. that has no conflict of interest related to the contents of this manuscripts. All the other authors declare no conflict of interest.
Figures
References
-
- Ito A., Miyoshi S., Toyota H., Suzuki Y., Uehara Y., Hattori S., Takeshita Y., Sakasegawa H., Kuramochi M., Kobayashi K., et al. The overlapping eligibility for biologics in patients with severe asthma and phenotypes. Arerugi. 2022;71:210–220. doi: 10.15036/arerugi.71.210. (In Japanese) - DOI - PubMed
LinkOut - more resources
Full Text Sources
