

Primary Cauda Equina Lymphoma Mimicking Meningioma
- PMID: 39201102
- PMCID: PMC11355680
- DOI: 10.3390/jcm13164959
Primary Cauda Equina Lymphoma Mimicking Meningioma
Abstract
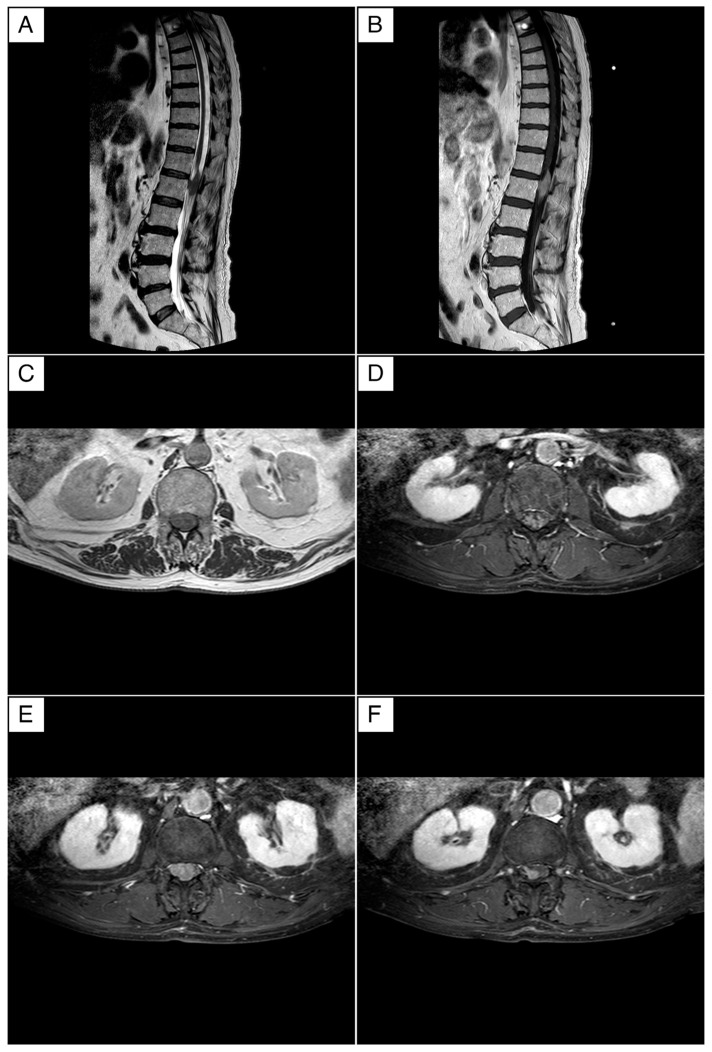
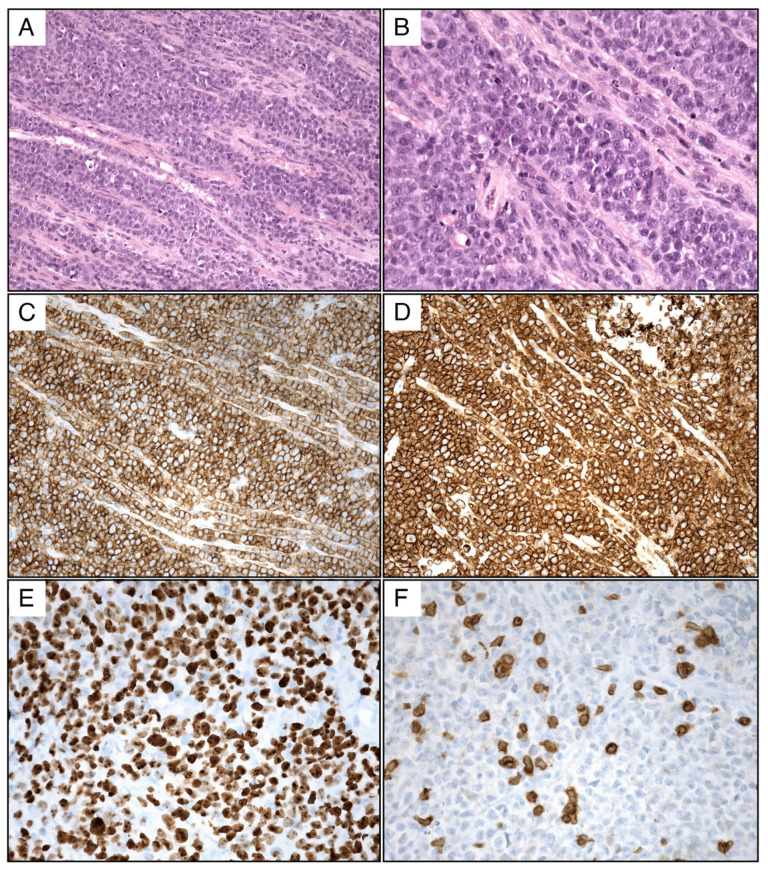
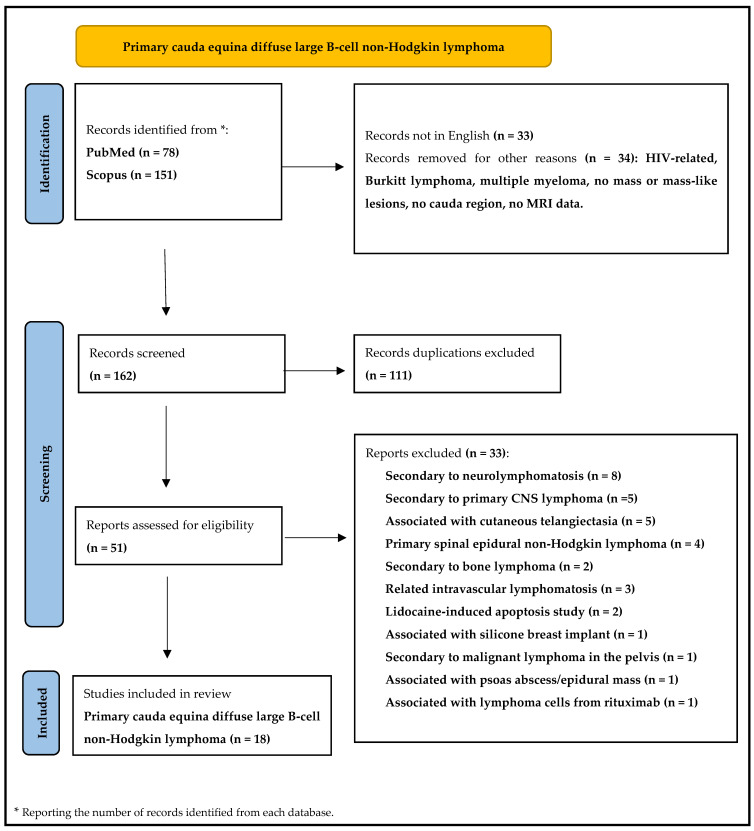
Background: Spinal cord lymphomas represent a minority of extranodal lymphomas and often pose diagnostic challenges by imitating primary spinal tumors or inflammatory/infective lesions. This paper presents a unique case of primary cauda equina lymphoma (PCEL) and conducts a comprehensive review to delineate the clinical and radiological characteristics of this rare entity. Case Report: A 74-year-old male presented with progressive paresthesia, motor weakness, and symptoms indicative of cauda equina syndrome. Neurological examination revealed paraparesis and sphincter dysfunction. Imaging studies initially suggested an intradural meningioma. However, surgical intervention revealed a diffuse large B-cell lymphoma infiltrating the cauda equina. Findings: A systematic review of the pertinent literature identified 18 primary cauda equina lymphoma cases. These cases exhibited diverse clinical presentations, treatments, and outcomes. The mean age at diagnosis was 61.25 years for women and 50 years for men, with an average follow-up of 16.2 months. Notably, 35% of patients were alive at 18 months, highlighting the challenging prognosis associated with PCEL. Discussion: Primary spinal cord lymphomas, especially within the cauda equina, remain rare and diagnostically complex due to their nonspecific clinical manifestations. The review highlights the need to consider spinal cord lymphoma in patients with neurological symptoms, even without a history of systemic lymphoma. Diagnostic Approaches: Magnetic resonance imaging (MRI) serves as the primary diagnostic tool but lacks specificity. Histopathological examination remains the gold standard for definitive diagnosis. The review underscores the importance of timely biopsy in suspected cases to facilitate accurate diagnosis and appropriate management. Management and Prognosis: Current management involves biopsy and chemotherapy; however, optimal treatment strategies remain ambiguous due to the rarity of PCEL. Despite aggressive therapeutic interventions, prognosis remains poor, emphasizing the urgency for enhanced diagnostic and treatment modalities. Conclusions: Primary cauda equina lymphoma poses diagnostic and therapeutic challenges, necessitating a high index of suspicion in patients with atypical spinal cord symptoms. Collaborative efforts between neurosurgical, oncological, and infectious diseases teams are imperative for timely diagnosis and management. Advancements in diagnostic precision and therapeutic options are crucial for improving patient outcomes.
Keywords: diagnostic challenges; diffuse large B-cell lymphoma; neurolymphomatosis; primary cauda equina lymphoma; spinal cord lesions; treatment outcomes.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
