

Effects of Community Assets on Major Health Conditions in England: A Data Analytic Approach
- PMID: 39201166
- PMCID: PMC11353348
- DOI: 10.3390/healthcare12161608
Effects of Community Assets on Major Health Conditions in England: A Data Analytic Approach
Abstract
Introduction: The broader determinants of health including a wide range of community assets are extremely important in relation to public health outcomes. Multiple health conditions, multimorbidity, is a growing problem in many populations worldwide.
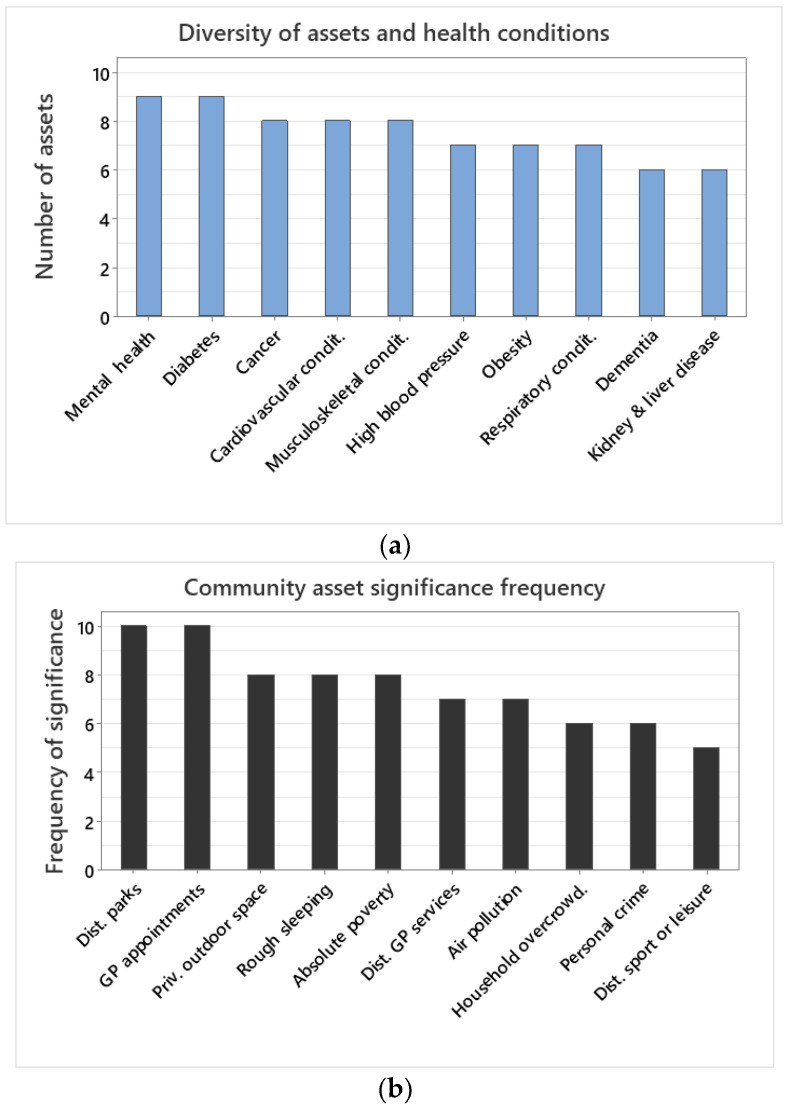
Methods: This paper quantified the effect of community assets on major health conditions for the population of England over six years, at a fine spatial scale using a data analytic approach. Community assets, which included indices of the health system, green space, pollution, poverty, urban environment, safety, and sport and leisure facilities, were quantified in relation to major health conditions. The health conditions examined included high blood pressure, obesity, dementia, diabetes, mental health, cardiovascular conditions, musculoskeletal conditions, respiratory conditions, kidney and liver disease, and cancer. Cluster analysis and dendrograms were calculated for the community assets and major health conditions. For each health condition, a statistical model with all community assets was fitted, and model selection was performed. The number of significant community assets for each health condition was recorded. The unique variance, explained by each significant community asset per health condition, was quantified using hierarchical variance partitioning within an analysis of variance model.
Results: The resulting data indicate major health conditions are often clustered, as are community assets. The results suggest that diversity and richness of community assets are key to major health condition outcomes. Primary care service waiting times and distance to public parks were significant predictors of all health conditions examined. Primary care waiting times explained the vast majority of the variances across health conditions, with the exception of obesity, which was better explained by absolute poverty.
Conclusions: The implications of the combined findings of the health condition clusters and explanatory power of community assets are discussed. The vast majority of determinants of health could be accounted for by healthcare system performance and distance to public green space, with important covariate socioeconomic factors. Emphases on community approaches, significant relationships, and asset strengths and deficits are needed alongside targeted interventions. Whilst the performance of the public health system remains of key importance, community assets and local infrastructure remain paramount to the broader determinants of health.
Keywords: community assets; data analytics; environmental health; green space; healthcare; multimorbidity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






References
-
- NIHR . Multiple Long-Term Conditions (Multimorbidity): Making Sense of the Evidence. Public Health; Bethesda, ML, USA: 2021. National Institute for Health and Care Research. - DOI
-
- GOV.UK Major Conditions Strategy: Case for Change and Our Strategic Framework. [(accessed on 20 February 2024)];Updated 21 August 2023. 2023 Available online: https://www.gov.uk/government/publications/major-conditions-strategy-cas....
-
- Healthcaredenmark Chronic Diseases and Multimorbidity in Denmark. 2023. [(accessed on 20 February 2024)]. Available online: https://healthcaredenmark.dk/news-publications/publications/chronic-dise...
-
- Struckmann V., Snoeijs S., Melchiorre M.G., Hujala A., Rijken M., Quentin W., van Ginneken E. Caring for people with multiple chronic conditions in Europe. Eurohealth. 2014;20:35–40.
Grants and funding
LinkOut - more resources
Full Text Sources
