

Normal Values for the fT3/fT4 Ratio: Centile Charts (0-29 Years) and Their Application for the Differential Diagnosis of Children with Developmental Delay
- PMID: 39201272
- PMCID: PMC11354987
- DOI: 10.3390/ijms25168585
Normal Values for the fT3/fT4 Ratio: Centile Charts (0-29 Years) and Their Application for the Differential Diagnosis of Children with Developmental Delay
Abstract
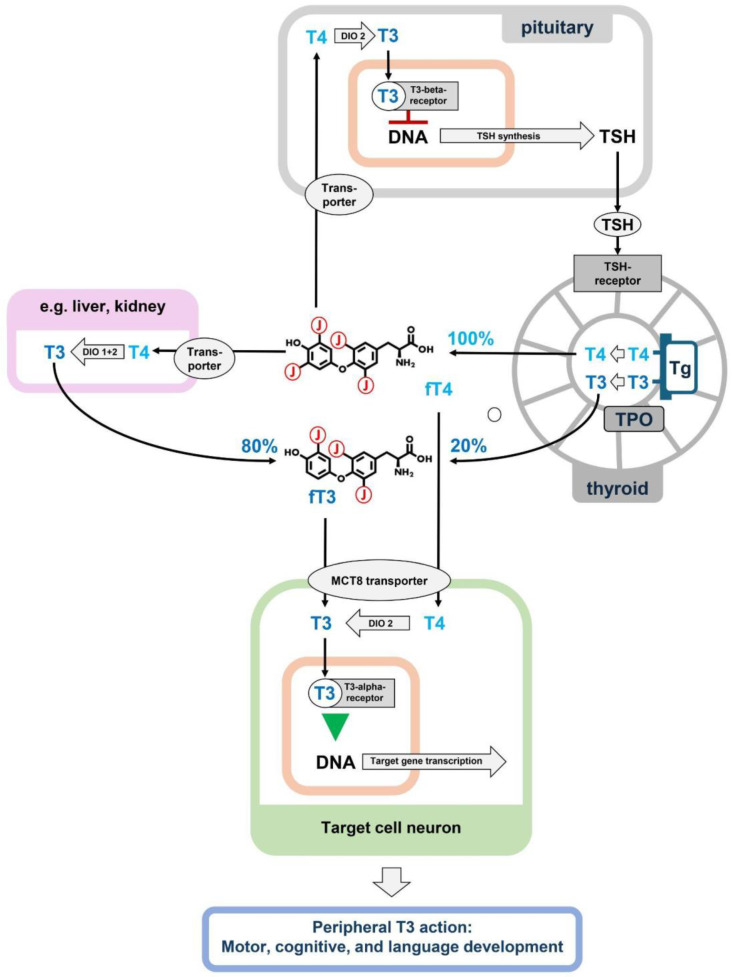
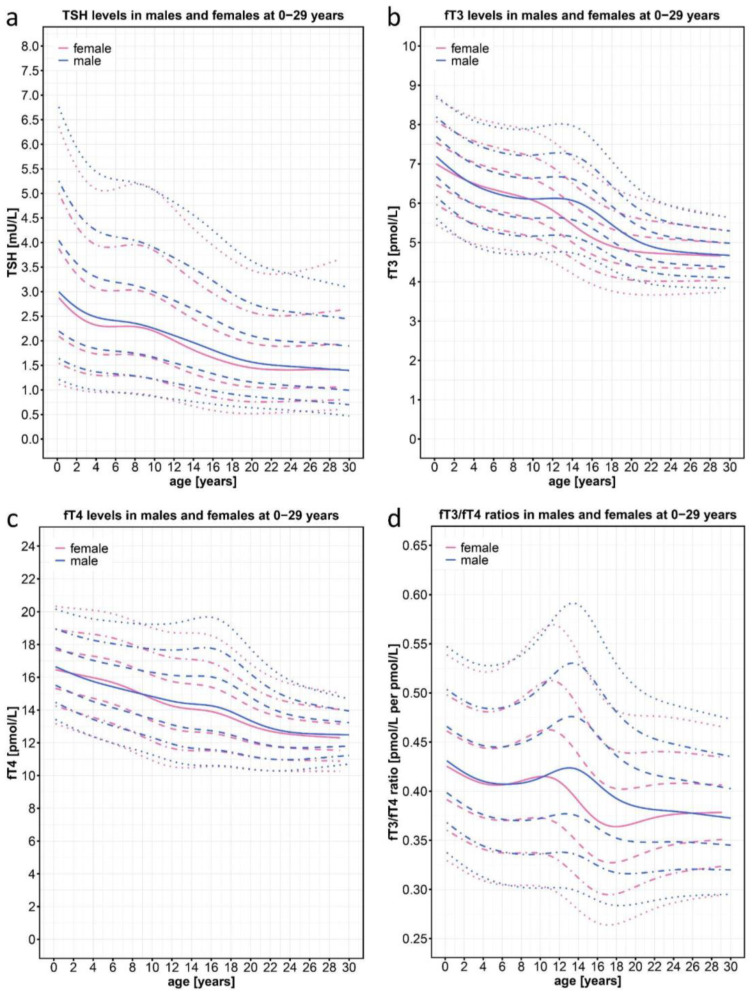
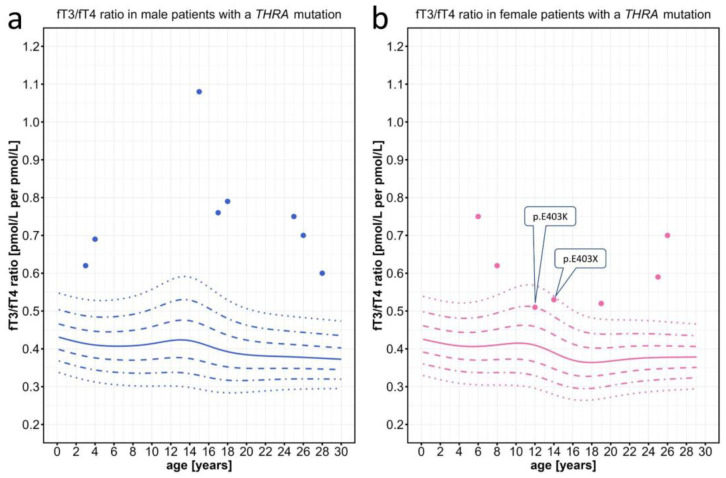
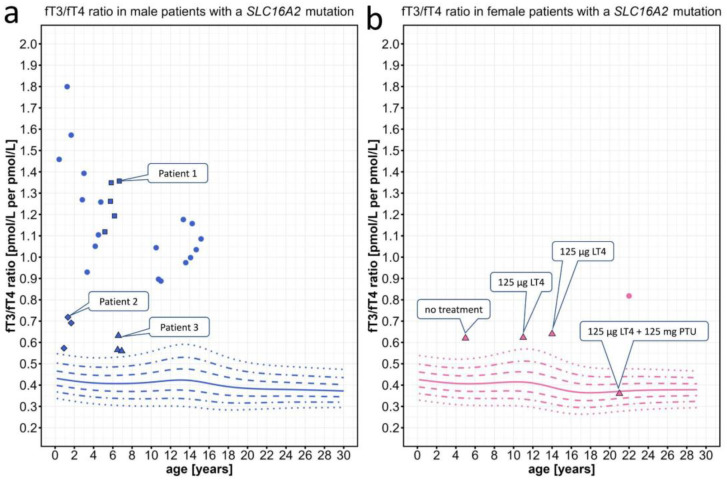
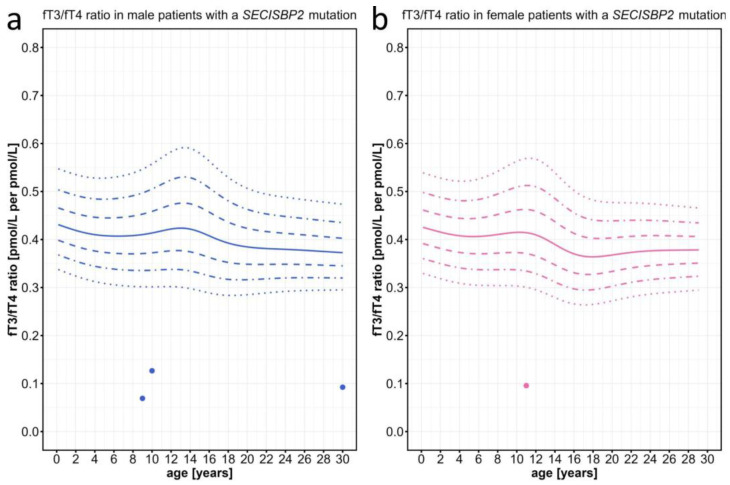
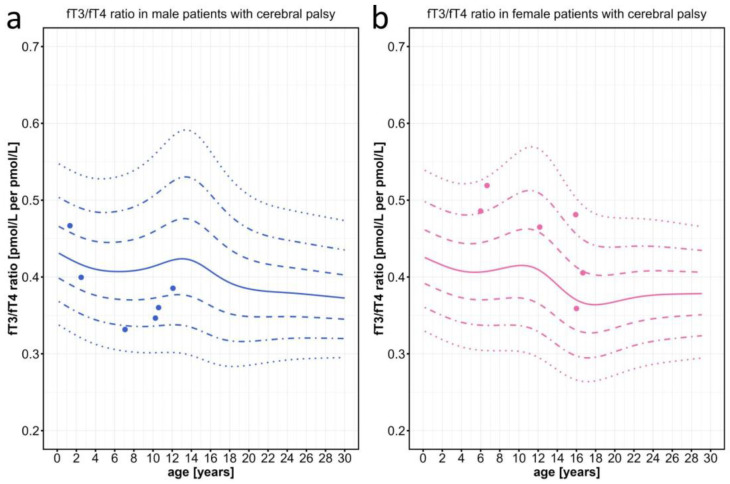
Primary congenital hypothyroidism is easily diagnosed on the basis of elevated plasma levels of thyroid-stimulating hormone (TSH). In contrast, in the rare disorders of thyroid hormone resistance, TSH and, in mild cases, also thyroid hormone levels are within the normal range. Thyroid hormone resistance is caused by defects in hormone metabolism, transport, or receptor activation and can have the same serious consequences for child development as congenital hypothyroidism. A total of n = 23,522 data points from a large cohort of children and young adults were used to generate normal values and sex-specific percentiles for the ratio of free triiodothyronine (T3) to free thyroxine (T4), the fT3/fT4 ratio. The aim was to determine whether individuals with developmental delay and genetically confirmed thyroid hormone resistance, carrying defects in Monocarboxylate Transporter 8 (MCT8), Thyroid Hormone Receptor alpha (THRα), and Selenocysteine Insertion Sequence-Binding Protein 2 (SECISBP2), had abnormal fT3/fT4 ratios. Indeed, we were able to demonstrate a clear separation of patient values for the fT3/fT4 ratio from normal and pathological controls (e.g., children with severe cerebral palsy). We therefore recommend using the fT3/fT4 ratio as a readily available screening parameter in children with developmental delay for the identification of thyroid hormone resistance syndromes. The fT3/fT4 ratio can be easily plotted on centile charts using our free online tool, which accepts various SI and non-SI units for fT3, fT4, and TSH.
Keywords: MCT8 deficiency; SECISBP2 mutations; SLC16A2 mutations; THRA mutations; TSH; fT3/fT4 ratio; peripheral thyroid hormone resistance; reference values; thyroid hormone.
Conflict of interest statement
N.M.W. has participated in a consultancy with Primus Consulting Group GmbH, advised the movie theater film production company Hellinger-Doll, and was paid by Biogen for a congress presentation. The funders had no role in the design of the study; in the collection, analysis, or interpretation of the data; in writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- van Trotsenburg P., Stoupa A., Léger J., Rohrer T., Peters C., Fugazzola L., Cassio A., Heinrichs C., Beauloye V., Pohlenz J., et al. Congenital Hypothyroidism: A 2020–2021 Consensus Guidelines Update—An ENDO-European Reference Network Initiative Endorsed by the European Society for Pediatric Endocrinology and the European Society for Endocrinology. Thyroid. 2021;31:387–419. doi: 10.1089/thy.2020.0333. - DOI - PMC - PubMed
-
- Aleksander P.E., Brückner-Spieler M., Stoehr A.-M., Lankes E., Kühnen P., Schnabel D., Ernert A., Stäblein W., Craig M.E., Blankenstein O., et al. Mean High-Dose l-Thyroxine Treatment Is Efficient and Safe to Achieve a Normal IQ in Young Adult Patients with Congenital Hypothyroidism. J. Clin. Endocrinol. Metab. 2018;103:1459–1469. doi: 10.1210/jc.2017-01937. - DOI - PubMed
MeSH terms
Substances
Grants and funding
- grant to Nina Maria Wilpert/Berliner Sparkassenstiftung Medizin
- TRR 296 P06 "Local control of TH action (LocoTact)"/Deutsche Forschungsgemeinschaft
- FOR2841/Deutsche Forschungsgemeinschaft
- Junior Clinician Scientist Program for Nina Maria Wilpert/Berlin Institute of Health at Charité - Universitätsmedizin Berlin
- EXC-2049-390688087 (NeuroCure)/Deutsche Forschungsgemeinschaft
LinkOut - more resources
Full Text Sources
Medical
