

New Biomarkers in Liver Fibrosis: A Pass through the Quicksand?
- PMID: 39201990
- PMCID: PMC11355846
- DOI: 10.3390/jpm14080798
New Biomarkers in Liver Fibrosis: A Pass through the Quicksand?
Abstract
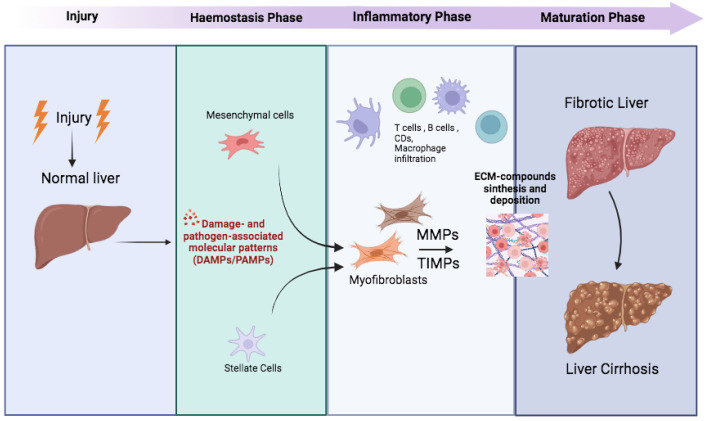
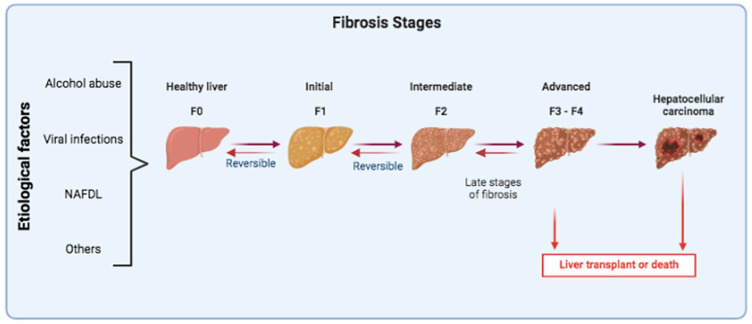
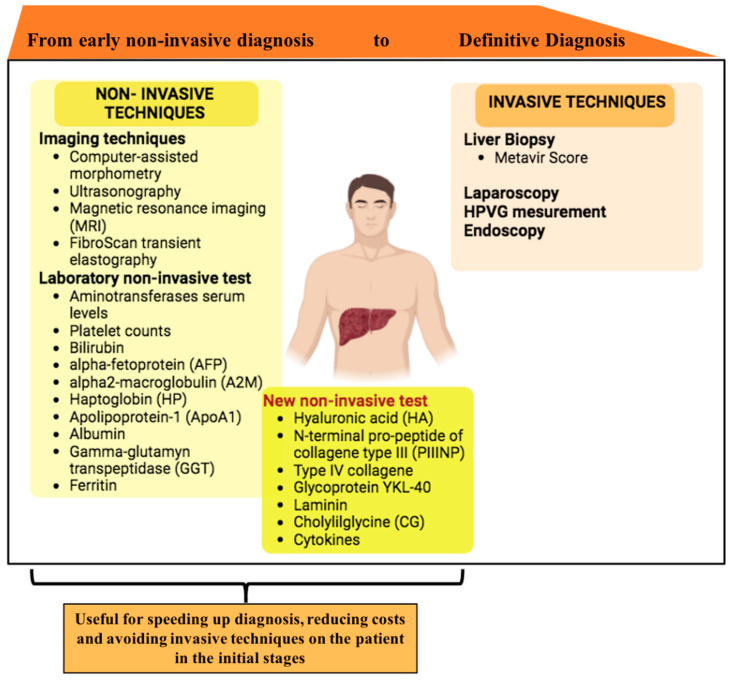
Chronic liver diseases (CLD) stem from various causes and lead to a gradual progression that ultimately may result in fibrosis and eventually cirrhosis. This process is typically prolonged and asymptomatic, characterized by the complex interplay among various cell types, signaling pathways, extracellular matrix components, and immune responses. With the prevalence of CLD increasing, diagnoses are often delayed, which leads to poor prognoses and in some cases, the need for liver transplants. Consequently, there is an urgent need for the development of novel, non-invasive methods for the diagnosis and monitoring of CLD. In this context, serum biomarkers-safer, repeatable, and more acceptable alternatives to tissue biopsies-are attracting significant research interest, although their clinical implementation is not yet widespread. This review summarizes the latest advancements in serum biomarkers for detecting hepatic fibrogenesis and advocates for concerted efforts to consolidate current knowledge, thereby providing patients with early, effective, and accessible diagnoses that facilitate personalized therapeutic strategies.
Keywords: biomarkers; extracellular matrix components; liver fibrosis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Vallonthaiel A.G., Baloda V., Singh L., Yadav R., Kilambi R., Battu S., Sreenivas V., Pal S., Acharya S.K., DattaGupta S., et al. Histological analyses of trucut liver biopsies from patients with noncirrhotic portal fibrosis and extra-hepatic portal vein obstruction. Indian J. Pathol. Microbiol. 2021;64((Suppl. 1)):S12–S135. doi: 10.4103/IJPM.IJPM_387_20. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
