

Intraoperative Fluorescent Navigation of the Ureters, Vessels, and Nerves during Robot-Assisted Sacrocolpopexy
- PMID: 39202018
- PMCID: PMC11355514
- DOI: 10.3390/jpm14080827
Intraoperative Fluorescent Navigation of the Ureters, Vessels, and Nerves during Robot-Assisted Sacrocolpopexy
Abstract
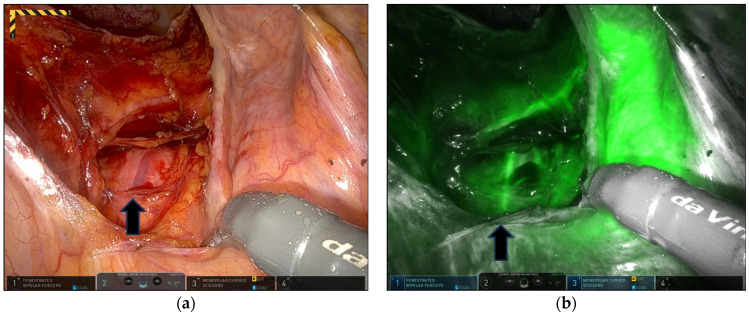
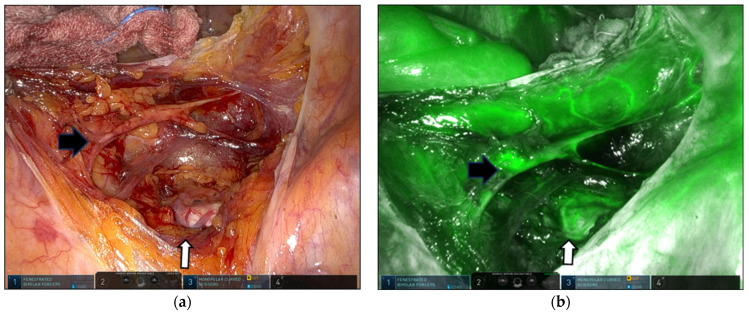
In this study, we aimed to demonstrate the feasibility and safety of navigating the ureters, middle sacral artery (MSA), and superior hypogastric nerve (SHN) using indocyanine green (ICG) and near-infrared fluorescence (NIRF) imaging during robot-assisted sacrocolpopexy (RSCP). Overall, 15 patients who underwent RSCP for apical vaginal prolapse were retrospectively enrolled. All patients underwent cystoscopic intraureteric instillation of 5 cc ICG (2.5 mg/mL) before RSCP and intravenous injection of 3 cc ICG during presacral dissection and mesh fixation. In all patients, the fluorescent right ureter was clearly identified in real time. The MSA was visualized on ICG-NIRF images in 80% (13/15) of patients. The mean time from ICG injection to MSA visualization was 43.7 s; the mean duration of the arterial phase was 104.3 s. Fluorescent SHN was detected in 73.3% (11/15) of patients. The time from ICG injection to SHN fluorescence was 48.4 s; the duration of fluorescence was 177.2 s. There was no transfusion, iatrogenic ureteral injury, or bowel or urinary dysfunction. Our results indicated that intraoperative ureter, MSA, and SHN mapping using ICG-NIRF images during RSCP is a valuable and safe technique to avoid iatrogenic ureteral, vascular, and neural injuries and to simplify surgical procedures. Nonetheless, further studies are required.
Keywords: apical vaginal prolapse; indocyanine green; middle sacral artery; near-infrared fluorescence imaging; real-time ureter; robot-assisted sacrocolpopexy; superior hypogastric nerve.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Intraoperative Fluorescent Ureter Visualization in Complex Laparoscopic or Robotic-Assisted Gynecologic Surgery.J Pers Med. 2023 Aug 31;13(9):1345. doi: 10.3390/jpm13091345. J Pers Med. 2023. PMID: 37763114 Free PMC article.
-
Use of indocyanine green during robot-assisted ureteral reconstructions.Eur Urol. 2015 Feb;67(2):291-8. doi: 10.1016/j.eururo.2014.08.057. Epub 2014 Sep 12. Eur Urol. 2015. PMID: 25220372
-
Indocyanine green for intraoperative localization of ureter.Am J Obstet Gynecol. 2014 Oct;211(4):436.e1-2. doi: 10.1016/j.ajog.2014.05.017. Epub 2014 May 14. Am J Obstet Gynecol. 2014. PMID: 24835212
-
Currently available and experimental dyes for intraoperative near-infrared fluorescence imaging of the ureters: a systematic review.Tech Coloproctol. 2019 Apr;23(4):305-313. doi: 10.1007/s10151-019-01973-4. Epub 2019 Apr 27. Tech Coloproctol. 2019. PMID: 31030340 Free PMC article.
-
Applications of Indocyanine Green-Guided Near-Infrared Fluorescence Imaging in Pediatric Minimally Invasive Surgery Urology: A Narrative Review.J Laparoendosc Adv Surg Tech A. 2022 Dec;32(12):1280-1287. doi: 10.1089/lap.2022.0231. Epub 2022 Nov 25. J Laparoendosc Adv Surg Tech A. 2022. PMID: 36450121 Review.
References
-
- Haylen B.T., Maher C.F., Barber M.D., Camargo S., Dandolu V., Digesu A., Goldman H.B., Huser M., Milani A.L., Moran P.A., et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP) Int. Urogynecol. J. 2016;27:655–684. doi: 10.1007/s00192-016-3003-y. - DOI - PubMed
-
- Schulten S.F.M., Claas-Quax M.J., Weemhoff M., van Eijndhoven H.W., van Leijsen S.A., Vergeldt T.F., IntHout J., Kluivers K.B. Risk factors for primary pelvic organ prolapse and prolapse recurrence: An updated systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2022;227:192–208. doi: 10.1016/j.ajog.2022.04.046. - DOI - PubMed
LinkOut - more resources
Full Text Sources
