

Opioid-Free Using Ketamine versus Opioid-Sparing Anesthesia during the Intraoperative Period in Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Trial
- PMID: 39202072
- PMCID: PMC11355072
- DOI: 10.3390/jpm14080881
Opioid-Free Using Ketamine versus Opioid-Sparing Anesthesia during the Intraoperative Period in Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Trial
Abstract
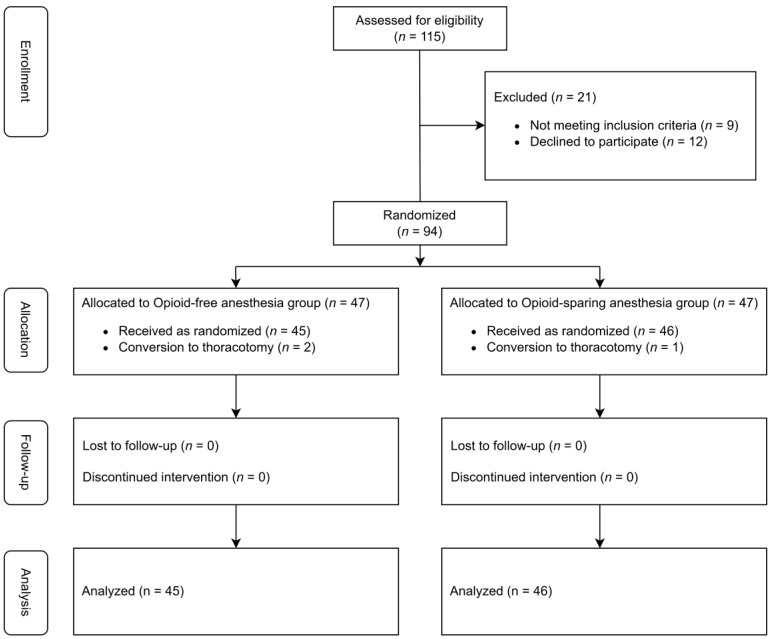
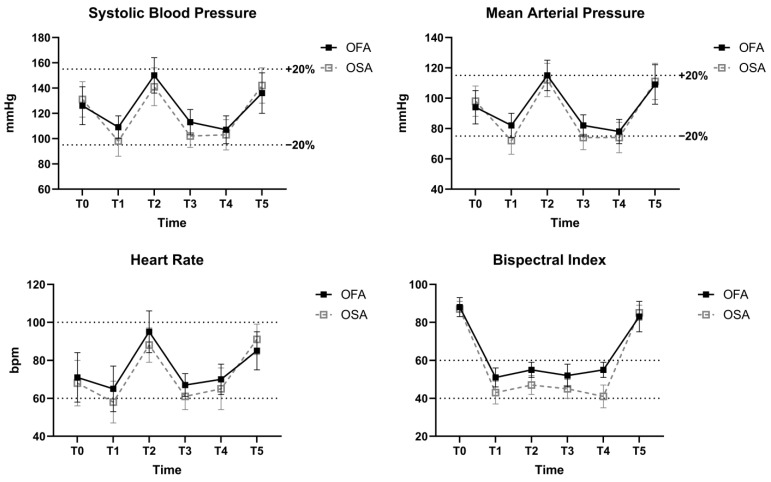
Opioids effectively manage perioperative pain but have numerous adverse effects. Opioid-free anesthesia (OFA) eliminates intraoperative opioid use; however, evidence for its use in video-assisted thoracoscopic surgery (VATS) is limited. This study assessed the effect of OFA using ketamine in VATS patients compared to opioid-sparing anesthesia (OSA). A total of 91 patients undergoing VATS lobectomy or segmentectomy were randomized to either the OFA group (ketamine) or the OSA group (remifentanil). The primary outcome was the quality of recovery (QoR) on postoperative day (POD) 1, measured with the QoR-40 questionnaire. Secondary outcomes included postoperative pain scores and adverse events. Both groups had comparable baseline and surgical characteristics. On POD 1, the QoR-40 score was higher in the OFA group than in the OSA group (164.3 ± 10.8 vs. 158.7 ± 10.6; mean difference: 5.6, 95% CI: 1.1, 10.0; p = 0.015), though this did not meet the pre-specified minimal clinically important difference of 6.3. The visual analog scale score was lower in the OFA group as compared to the OSA group at 0-1 h (4.2 ± 2.3 vs. 6.2 ± 2.1; p < 0.001) and 1-4 h after surgery (3.4 ± 1.8 vs. 4.6 ± 1.9; p = 0.003). The OFA group had a lower incidence of PONV (2 [4.4%] vs. 9 [19.6%]; p = 0.049) and postoperative shivering (4 [8.9%] vs. 13 [28.3%]; p = 0.030) than the OSA group at 0-1 h after surgery. Using OFA with ketamine proved feasible, as indicated by the stable intraoperative hemodynamics and absence of intraoperative awareness. Patients undergoing VATS with OFA using ketamine showed a statistically significant, but clinically insignificant, QoR improvement compared to those receiving OSA with remifentanil.
Keywords: opioid; opioid-free anesthesia; opioid-sparing anesthesia; thoracic anesthesia.
Conflict of interest statement
The authors declare no conflicts of interest. The funder played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
