

Advancing the Diagnosis of Diabetic Neuropathies: Electrodiagnostic and Skin Autofluorescence Methods
- PMID: 39202075
- PMCID: PMC11355645
- DOI: 10.3390/jpm14080884
Advancing the Diagnosis of Diabetic Neuropathies: Electrodiagnostic and Skin Autofluorescence Methods
Abstract
Introduction: Diabetic neuropathy (DN) is a generic term for various neuropathies coexisting in a single patient. Clinical diagnosis alone can be misleading, yet routine electrodiagnostic studies in diabetes care are rare. Skin autofluorescence (SAF) is a recognized DN risk factor with potential screening value. This article highlights the diagnostic challenges and raises awareness of the often underdiagnosed neuropathic conditions in diabetes patients.
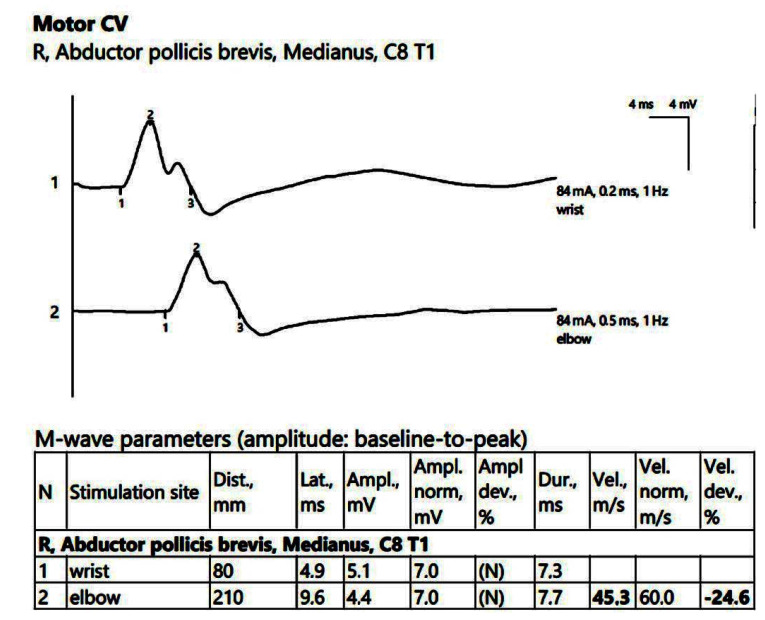
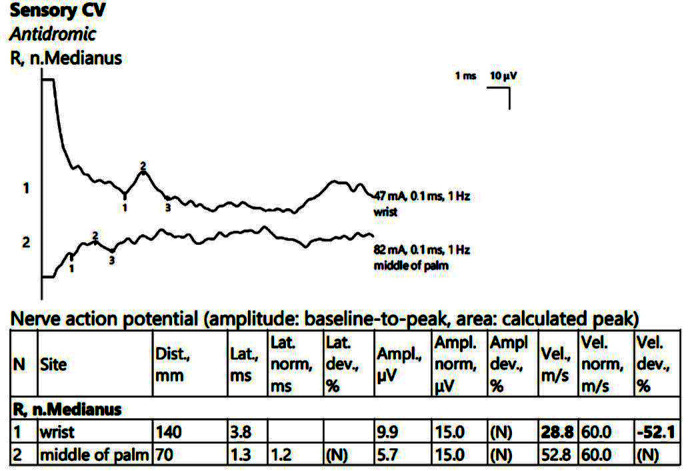
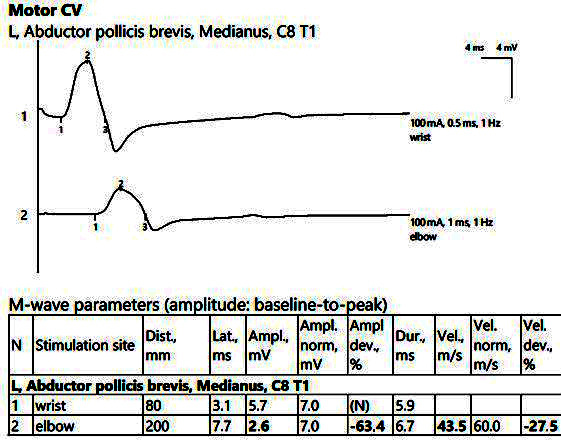
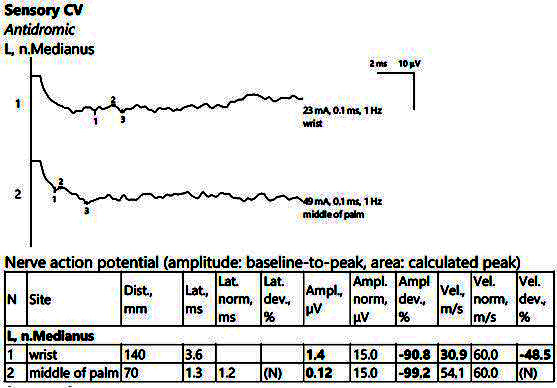
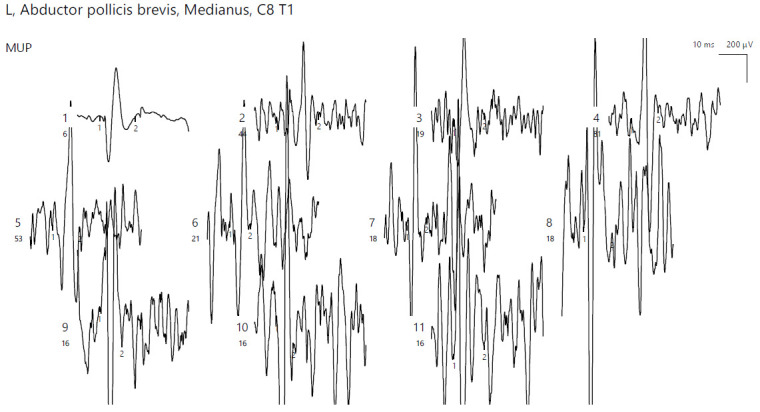
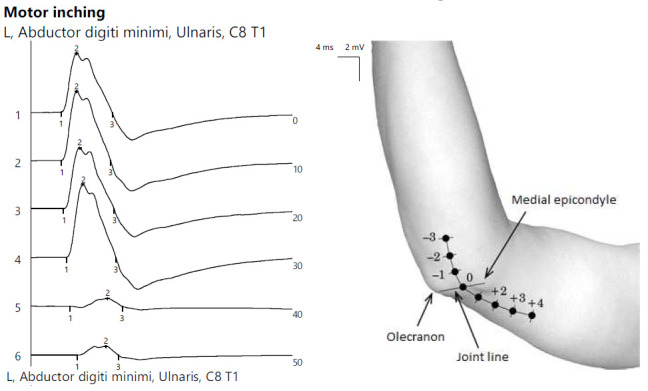
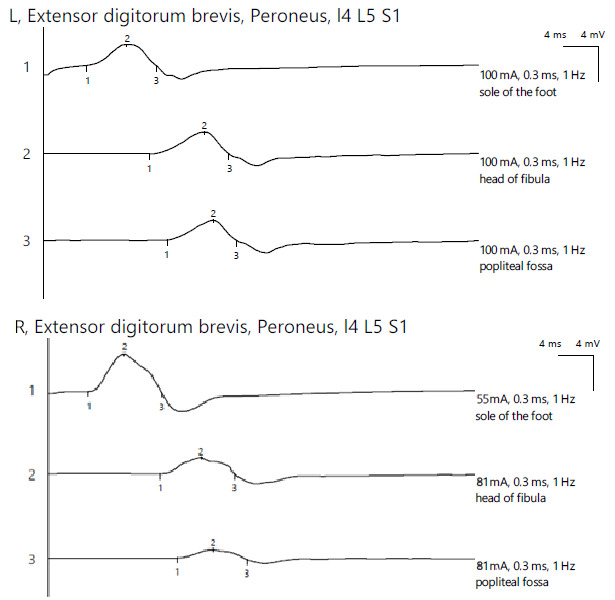
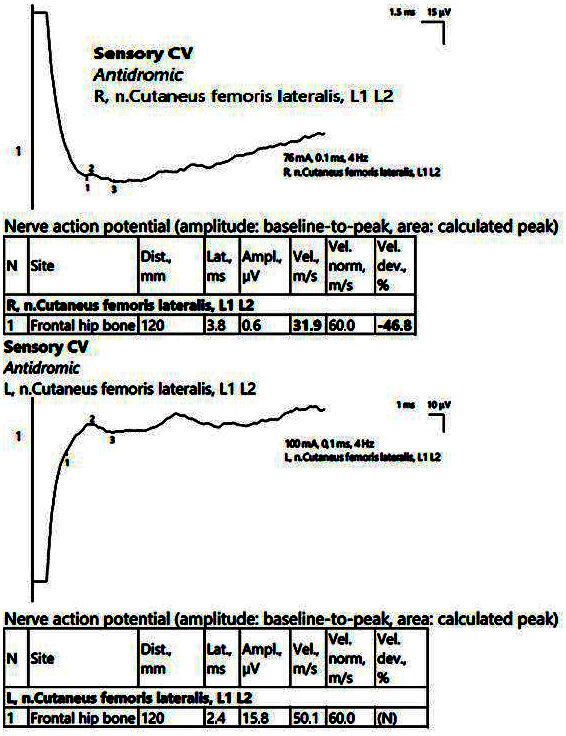
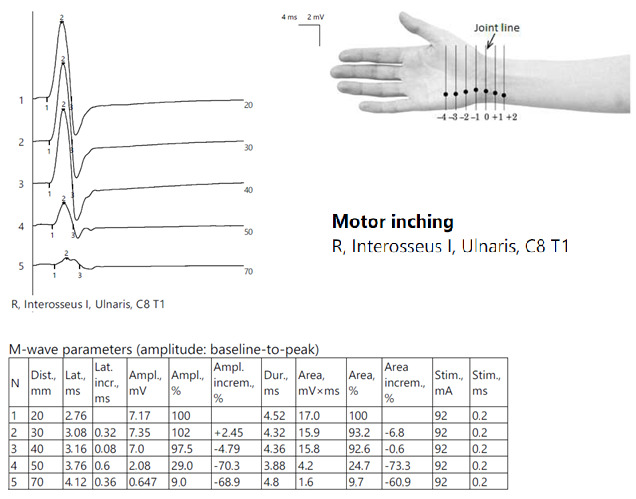
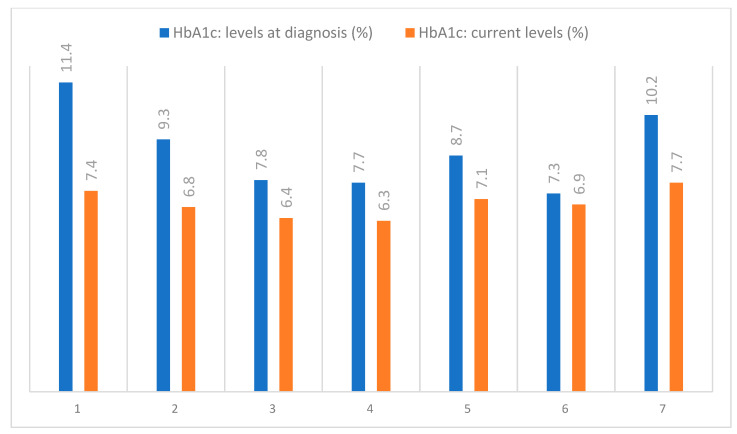
Material and methods: We present common entrapment neuropathy cases from our diabetes clinic's electrodiagnosis laboratory in Iași, Romania. We selected seven type 2 diabetes patients with sensory or sensory-motor distal polyneuropathy and atypical DN presentations investigated through electroneurography (ENG) and electromyography (EMG) with the Neurosoft® EMG instrument and SAF measured by standard procedures. Subsequently, a narrative literature review was conducted.
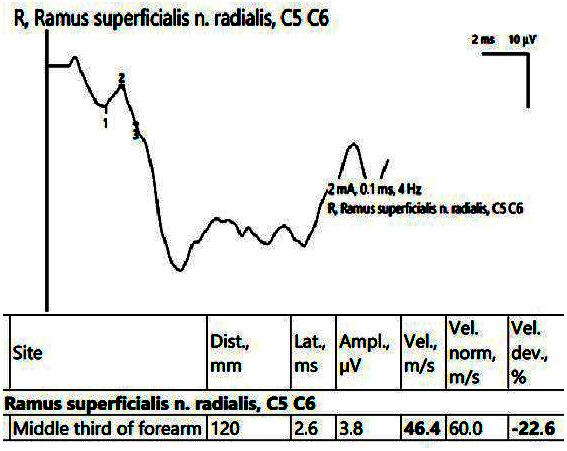
Results: Entrapment neuropathies were diagnosed in all the patients: three carpal tunnel syndromes, two ulnar neuropathies (one proximal, one distal), one peroneal neuropathy, and one case of meralgia paresthetica. The lower-limb cases showed radiculoplexopathy, and there was one case of superficial radial nerve neuropathy. The SAF values ranged from 2.5 AU to 3.4 AU.
Conclusions: Electrodiagnosis is essential for detecting focal neuropathies in patients with sensory-motor distal polyneuropathy. Elevated SAF levels may correlate with symptom severity, although further research, including large cohorts, is needed.
Keywords: AGEs; HbA1c; electroneurography; entrapment neuropathy; skin autofluorescence.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Electrodiagnostic testing in diabetic neuropathy: Which limb?Diabetes Res Clin Pract. 2015 Oct;110(1):95-97. doi: 10.1016/j.diabres.2015.07.009. Epub 2015 Aug 1. Diabetes Res Clin Pract. 2015. PMID: 26272740
-
Ulnar entrapment neuropathy in patients with type 2 diabetes mellitus: an electrodiagnostic study.Diabetes Res Clin Pract. 2014 Apr;104(1):73-8. doi: 10.1016/j.diabres.2014.01.024. Epub 2014 Feb 3. Diabetes Res Clin Pract. 2014. PMID: 24565211
-
Diagnostic Approach to Lower Limb Entrapment Neuropathies: A Narrative Literature Review.Diagnostics (Basel). 2023 Nov 4;13(21):3385. doi: 10.3390/diagnostics13213385. Diagnostics (Basel). 2023. PMID: 37958280 Free PMC article. Review.
-
Skin Autofluorescence Is Associated with Diabetic Peripheral Neuropathy in Chinese Patients with Type 2 Diabetes: A Cross-Sectional Study.Genet Test Mol Biomarkers. 2019 Jun;23(6):387-392. doi: 10.1089/gtmb.2018.0328. Genet Test Mol Biomarkers. 2019. PMID: 31161820 Free PMC article.
-
Electrodiagnostic Testing of Entrapment Neuropathies: A Review of Existing Guidelines.J Clin Neurophysiol. 2020 Jul;37(4):299-305. doi: 10.1097/WNP.0000000000000668. J Clin Neurophysiol. 2020. PMID: 33151661 Review.
Cited by
-
Could Skin Autofluorescence Be a Useful Biomarker in Systemic Lupus Erythematosus? A Systematic Review.Int J Mol Sci. 2025 Jul 19;26(14):6934. doi: 10.3390/ijms26146934. Int J Mol Sci. 2025. PMID: 40725181 Free PMC article.
References
-
- Lupescu D.T. Neuropatia Diabetică. Editura Viața Medicală; Bucharest, Romania: 2016. Electrodiagnosticul în neuropatia diabetică; pp. 40–43.
-
- Hermányi P., Kempler P. Types, clinical picture, and diagnosis of somatic neuropathy. In: Kempler P., Varkonyi T., editors. Neuropathies. A Global Clinical Guide. Volume 3. Zafir Press; Budapest, Hungary: 2012.
-
- Preston D.C., Shapiro D.E. Electromyography and Neuromuscular Disorders: Clinical–Electrophysiologic Correlations. Volume 6. Elsevier Inc.; Amsterdam, The Netherlands: 2013.
-
- Glenn M.D., Jabari D. Diabetic Lumbosacral Radiculoplexus Neuropathy (Diabetic Amyotrophy) Neurol. Clin. 2020;38:553–564. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
