

Computed Tomography of Contemporary Occupational Lung Disease: A Pictorial Review
- PMID: 39202274
- PMCID: PMC11353255
- DOI: 10.3390/diagnostics14161786
Computed Tomography of Contemporary Occupational Lung Disease: A Pictorial Review
Abstract
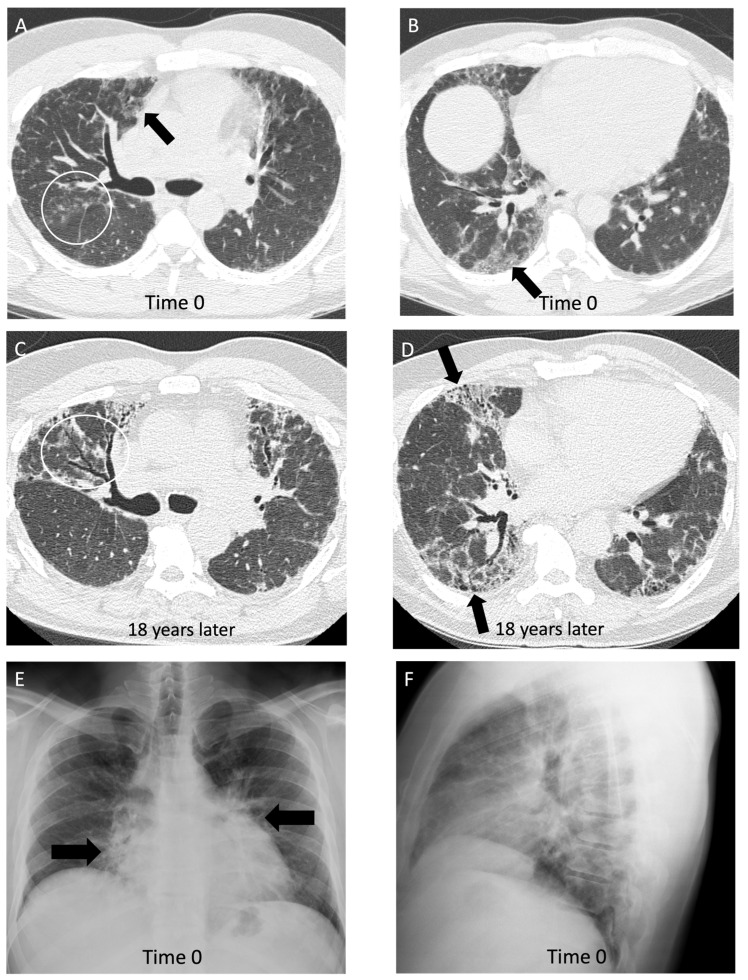
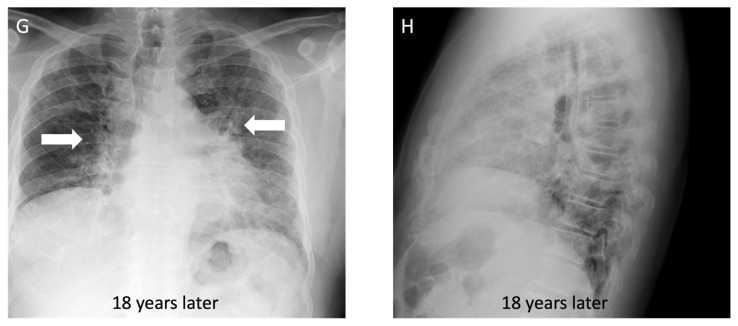
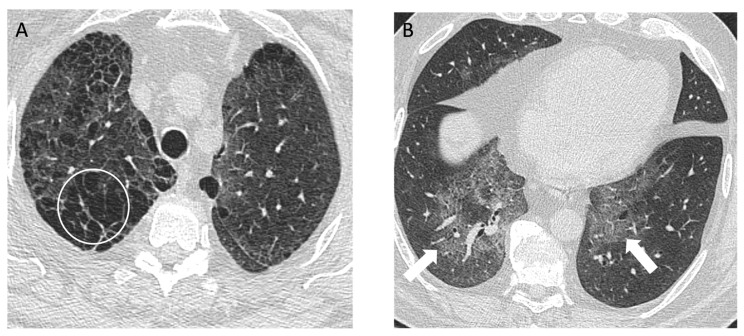
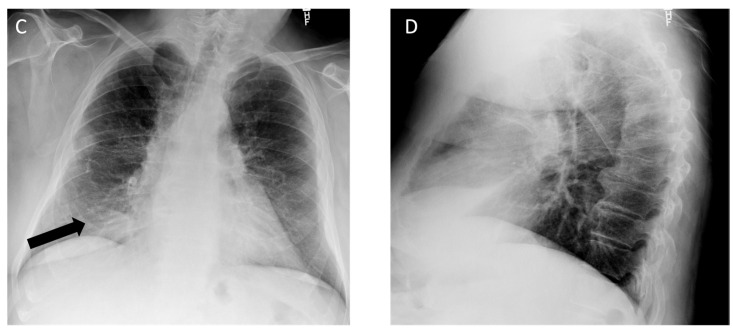
Occupational lung disease remains one of the most common work-related illnesses and accounts for most deaths from occupational illness. Occupational lung diseases often have delayed manifestation over decades and nonspecific clinical presentations, making it challenging for clinicians to promptly identify the disease and implement preventive measures. Radiologists play a crucial role in identifying and diagnosing occupational lung diseases, allowing for removal of the exposure and early medical intervention. In this review, we share our clinical and radiologic approach to diagnosing occupational lung disease and its subtypes. A collection of sample cases of occupational lung diseases commonly encountered in the modern era at a large Canadian university hospital is included to facilitate understanding. This review will provide radiologists with valuable insights into recognizing and diagnosing occupational lung diseases.
Keywords: asbestosis; hypersensitivity pneumonitis; occupational lung disease; pneumoconiosis; silicosis; work-related asthma.
Conflict of interest statement
M.M. reports consulting fees from AstraZeneca and honoraria from Boehringer Ingelheim, unrelated to the current work. All other authors declare no relevant relationships.
Figures
Similar articles
-
Inhalational lung diseases.Radiologia (Engl Ed). 2022 Dec;64 Suppl 3:290-300. doi: 10.1016/j.rxeng.2022.10.007. Radiologia (Engl Ed). 2022. PMID: 36737167
-
Imaging of occupational lung disease.Radiographics. 2001 Nov-Dec;21(6):1371-91. doi: 10.1148/radiographics.21.6.g01nv011371. Radiographics. 2001. PMID: 11706211 Review.
-
Occupational Lung Diseases: Spectrum of Common Imaging Manifestations.Korean J Radiol. 2023 Aug;24(8):795-806. doi: 10.3348/kjr.2023.0274. Korean J Radiol. 2023. PMID: 37500580 Free PMC article. Review.
-
Less Common Respiratory Conditions: Occupational Lung Diseases.FP Essent. 2021 Mar;502:11-17. FP Essent. 2021. PMID: 33683849
-
[Diffuse interstitial lung disease of possible occupational origin treated at the Navarra Health Service. Navarra, Spain, 2017-2022].Arch Prev Riesgos Labor. 2024 Apr 15;27(2):173-189. doi: 10.12961/aprl.2024.27.02.05. Arch Prev Riesgos Labor. 2024. PMID: 38655592 Spanish.
References
-
- Blanc P.D., Annesi-Maesano I., Balmes J.R., Cummings K.J., Fishwick D., Miedinger D., Murgia N., Naidoo R.N., Reynolds C.J., Sigsgaard T., et al. The Occupational Burden of Nonmalignant Respiratory Diseases. An Official American Thoracic Society and European Respiratory Society Statement. Am. J. Respir. Crit. Care Med. 2019;199:1312–1334. doi: 10.1164/rccm.201904-0717ST. - DOI - PMC - PubMed
-
- Hoy R.F., Jeebhay M.F., Cavalin C., Chen W., Cohen R.A., Fireman E., Go L.H.T., León-Jiménez A., Menéndez-Navarro A., Ribeiro M., et al. Current global perspectives on silicosis—Convergence of old and newly emergent hazards. Respirology. 2022;27:387–398. doi: 10.1111/resp.14242. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
