

Effectiveness of Apparent Diffusion Coefficient Values in Predicting Pathologic Subtypes and Grade in Non-Small-Cell Lung Cancer
- PMID: 39202283
- PMCID: PMC11354131
- DOI: 10.3390/diagnostics14161795
Effectiveness of Apparent Diffusion Coefficient Values in Predicting Pathologic Subtypes and Grade in Non-Small-Cell Lung Cancer
Abstract
Background and objective: The aim of this study is to evaluate the effectiveness of apparent diffusion coefficient (ADC) values in predicting pathologic subtypes and grade in non-small-cell lung cancer (NSCLC).
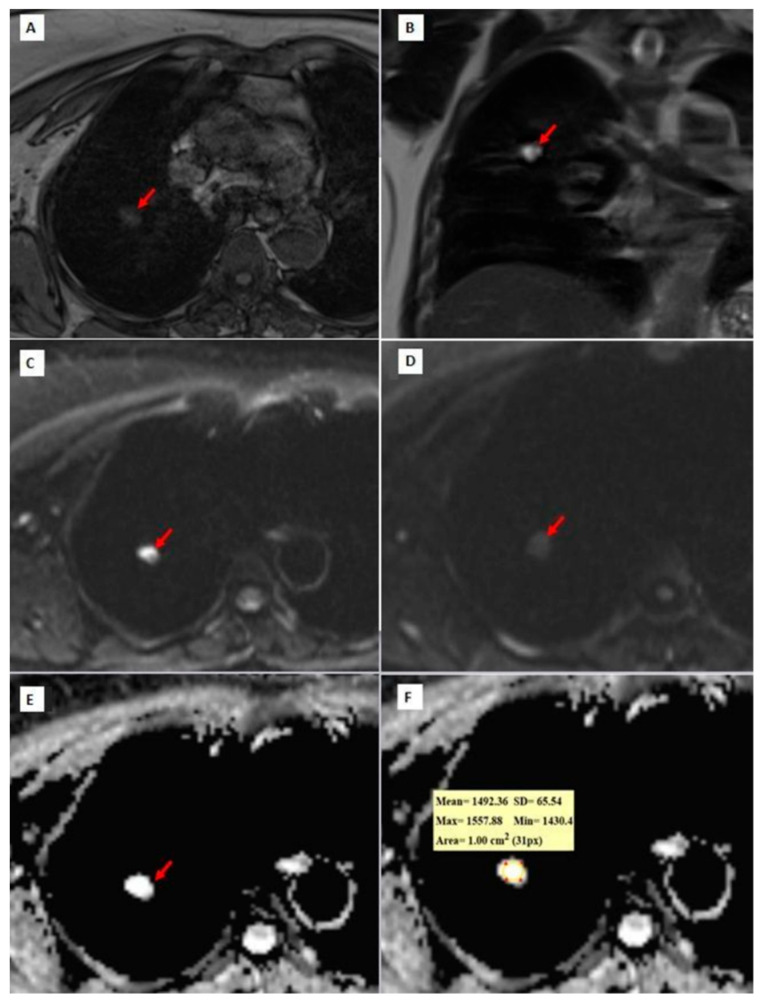
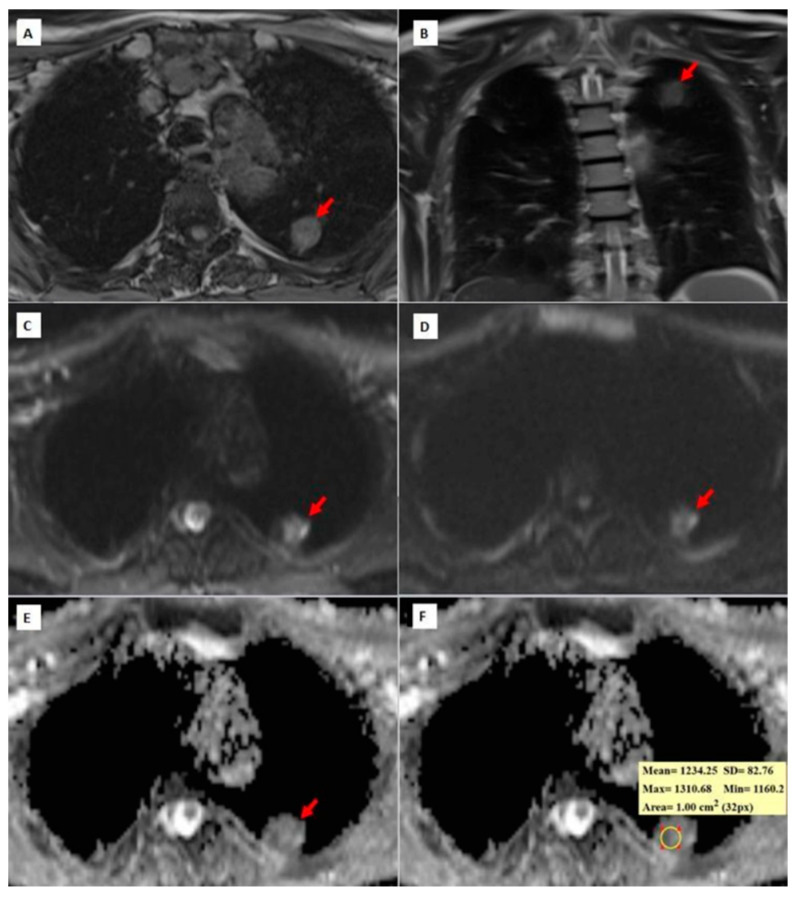
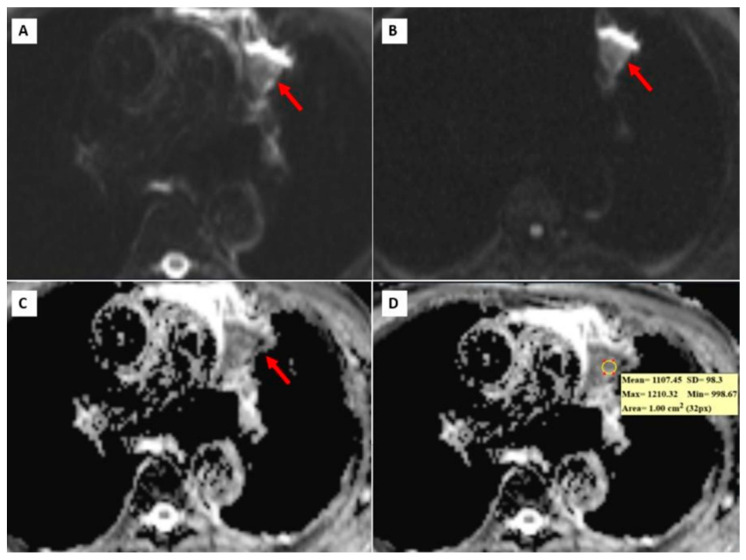
Materials and methods: From January 2018 to March 2020, 48 surgically diagnosed NSCLC cases were included in this study. To obtain ADC values, ADC maps were constructed, and a region of interest was put on the tumor. The values were measured three times from different places of the lesion, and the mean value of these measurements was recorded. All MRI scans were evaluated by two radiologists in consensus.
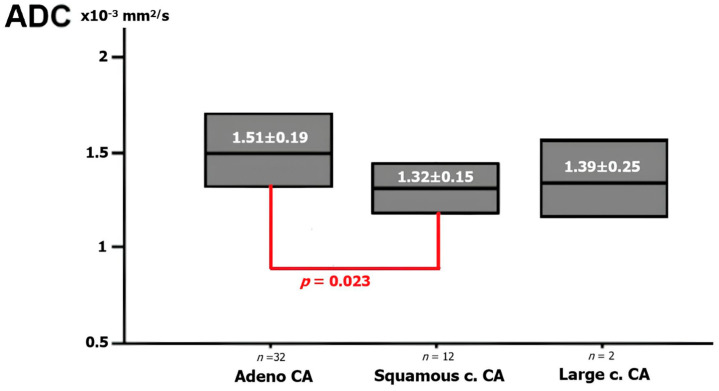
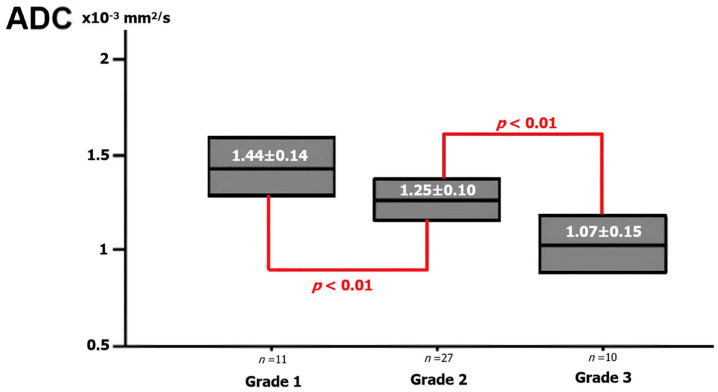
Results: A total of 14 cases were squamous cell cancer, 32 cases were adenocarcinoma, and 2 cases were large cell carcinoma. The mean ADC values of adenocarcinoma, squamous cell carcinoma, and large cell cancer were 1.51 ± 0.19 × 10-3 mm2/s, 1.32 ± 0.15 × 10-3 mm2/s, and 1.39 ± 0.25 × 10-3 mm2/s, respectively. There were 11 grade 1, 27 grade 2, and 10 grade 3 NSCLC cases. The mean ADC value was 1.44 ± 0.14 × 10-3 mm2/s in grade 1 tumors, 1.25 ± 0.10 × 10-3 mm2/s in grade 2 tumors, and 1.07 ± 0.15 × 10-3 mm2/s in grade 3 tumors. The cut-off value to discriminate grade 2 from grade 1 tumors was 1.31 ± 0.11 × 10-3 mm2/s (85% sensitivity, 75% specificity). The cut-off value to discriminate grade 3 from grade 2 tumors was 1.11 ± 0.15 × 10-3 mm2/s (87% sensitivity, 69% specificity).
Conclusions: ADC values can accurately predict NSCLC histopathologic subtypes and tumor grade.
Keywords: ADC value; diffusion-weighted imaging; lung adenocarcinoma; non-small-cell lung cancer; squamous cell lung cancer; tumor grade.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Can diffusion-weighted magnetic resonance imaging of clear cell renal carcinoma predict low from high nuclear grade tumors.Abdom Radiol (NY). 2017 Apr;42(4):1241-1249. doi: 10.1007/s00261-016-0981-7. Abdom Radiol (NY). 2017. PMID: 27904923
-
Differential diagnosis of the small renal masses: role of the apparent diffusion coefficient of the diffusion-weighted MRI.Int Urol Nephrol. 2018 Feb;50(2):197-204. doi: 10.1007/s11255-017-1761-1. Epub 2017 Dec 11. Int Urol Nephrol. 2018. PMID: 29230706
-
Non-small cell lung cancer: Whole-lesion histogram analysis of the apparent diffusion coefficient for assessment of tumor grade, lymphovascular invasion and pleural invasion.PLoS One. 2017 Feb 16;12(2):e0172433. doi: 10.1371/journal.pone.0172433. eCollection 2017. PLoS One. 2017. PMID: 28207858 Free PMC article.
-
Diffusion-weighted MRI in renal cell carcinoma: a surrogate marker for predicting nuclear grade and histological subtype.Acta Radiol. 2012 Apr 1;53(3):349-58. doi: 10.1258/ar.2011.110415. Acta Radiol. 2012. PMID: 22496427
-
Relationships and Qualitative Evaluation Between Diffusion-Weighted Imaging and Pathologic Findings of Resected Lung Cancers.Cancers (Basel). 2020 May 8;12(5):1194. doi: 10.3390/cancers12051194. Cancers (Basel). 2020. PMID: 32397172 Free PMC article.
References
-
- Global Cancer Observatory: Cancer Today. International Agency for Research on Cancer; Lyon, France: [(accessed on 15 September 2020)]. Available online: https://gco.iarc.fr/today.
LinkOut - more resources
Full Text Sources
