

Bioresorbable Scaffold Use in Coronary Chronic Total Occlusions: A Long-Term, Single-Center Follow-Up Study
- PMID: 39202514
- PMCID: PMC11356204
- DOI: 10.3390/medicina60081233
Bioresorbable Scaffold Use in Coronary Chronic Total Occlusions: A Long-Term, Single-Center Follow-Up Study
Abstract
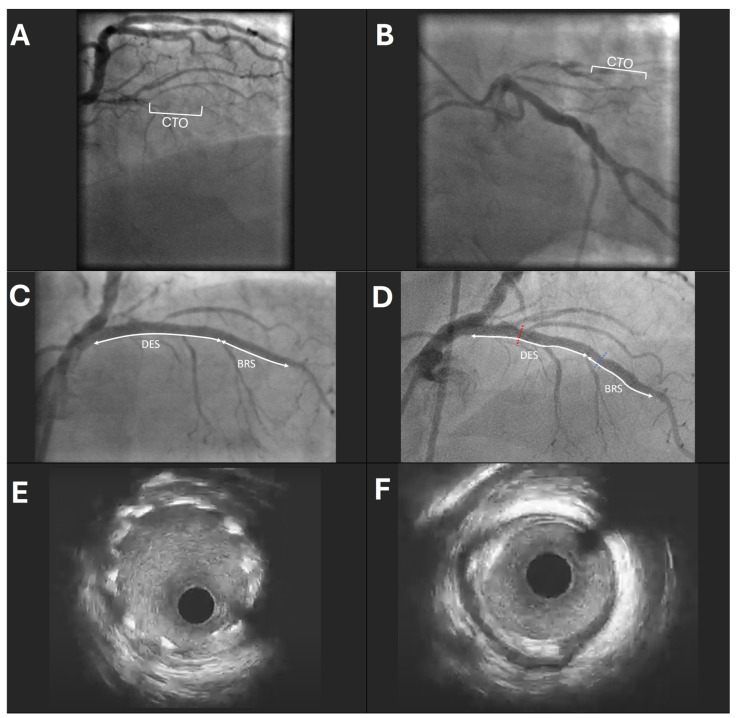
Background and Objectives: Percutaneous coronary intervention (PCI) of chronic total occlusion (CTO) is often associated with longer total stent length. Our aim was to evaluate the long-term safety and effectiveness of bioresorbable scaffold (BRS) implantation in CTO to avoid using a full metal jacket. Materials and Methods: We conducted a single-center prospective longitudinal case study including 34 patients who underwent PCI of CTO with at least one BRS and drug-eluting stent (DES) implantation (n = 27) or BRS-only at the Latvian Centre of Cardiology between 2016 and 2018. Quantitative coronary angiography (QCA) and intravascular ultrasound were performed during the index procedure and long-term follow-up. Results: Of 34 patients with a mean age of 60.6 ± 9.5 years, 76.5% were male. The most common CTO artery was the right coronary artery (73.5%, n = 25). The median length of occlusion was 23.0 mm (interquartile range (IQR) = 13.9-32.7), with a total mean BRS/DES length of 49.6 ± 20.4 mm. During the median follow-up of 5.6 years (IQR = 5.0-5.9), the primary endpoint of target vessel re-occlusion occurred in 5.9% (n = 2) of patients. Target lesion revascularization (TLR) was performed in 35.3% (n = 12) of patients, with a mean time to TLR of 62.5 (95% confidence interval (CI), 53.9-71.2) months. Through QCA, there was a statistically significant increase in median residual diameter stenosis (20.1-31.4%, p < 0.01) and residual length of stenosis (5.2-7.1%, p = 0.04) compared with the index procedure. Conclusions: Our study demonstrates that BRS is a safe and feasible option for PCI of CTO, allowing for the avoidance of long segment stenting and ensuring long-term patency of the coronary artery.
Keywords: bioresorbable scaffolds; chronic total occlusion; coronary artery disease; percutaneous coronary intervention.
Conflict of interest statement
The authors, except A.E., declare no conflicts of interest. Author A.E. has received speaker honorariums from Abbott Vascular and Biotronik.
Figures
References
-
- Ybarra L.F., Rinfret S., Brilakis E.S., Karmpaliotis D., Azzalini L., Grantham J.A., Kandzari D.E., Mashayekhi K., Spratt J.C., Wijeysundera H.C., et al. Definitions and Clinical Trial Design Principles for Coronary Artery Chronic Total Occlusion Therapies: CTO-ARC Consensus Recommendations. Circulation. 2021;143:479–500. doi: 10.1161/CIRCULATIONAHA.120.046754. - DOI - PubMed
-
- Werner G.S., Hildick-Smith D., Martin Yuste V., Boudou N., Sianos G., Gelev V., Rumoroso J.R., Erglis A., Christiansen E.H., Escaned J., et al. Three-year outcomes of A Randomized Multicentre Trial Comparing Revascularization and Optimal Medical Therapy for Chronic Total Coronary Occlusions (EuroCTO) EuroIntervention. 2023;19:571–579. doi: 10.4244/EIJ-D-23-00312. - DOI - PMC - PubMed
-
- Lee S.W., Lee P.H., Ahn J.M., Park D.W., Yun S.C., Han S., Kang H., Kang S.J., Kim Y.H., Lee C.W., et al. Randomized Trial Evaluating Percutaneous Coronary Intervention for the Treatment of Chronic Total Occlusion. Circulation. 2019;139:1674–1683. doi: 10.1161/CIRCULATIONAHA.118.031313. - DOI - PubMed
-
- Rha S.W., Choi B.G., Baek M.J., Ryu Y.G., Li H., Choi S.Y., Byun J.K., Mashaly A., Park Y., Jang W.Y., et al. Five-Year Outcomes of Successful Percutaneous Coronary Intervention with Drug-Eluting Stents versus Medical Therapy for Chronic Total Occlusions. Yonsei Med. J. 2018;59:602–610. doi: 10.3349/ymj.2018.59.5.602. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
