

Usefulness of Serum Testosterone Concentration and Skin Autofluorescence as Coronary Risk Markers in Male Patients With Type 2 Diabetes Mellitus
- PMID: 39205964
- PMCID: PMC11349139
- DOI: 10.14740/cr1686
Usefulness of Serum Testosterone Concentration and Skin Autofluorescence as Coronary Risk Markers in Male Patients With Type 2 Diabetes Mellitus
Abstract
Background: No studies have reported simultaneous evaluation of the two coronary risk markers of testosterone and skin autofluorescence (SAF) as a marker of advanced glycation end products in patients with type 2 diabetes mellitus (T2DM) at present. This study aimed to clarify the clinical significance of both indicators as risk markers of coronary artery disease (CAD), including the association and background factors between testosterone and SAF in male patients with T2DM.
Methods: This study enrolled 162 male patients with T2DM (CAD: n = 35). Testosterone was evaluated by serum total testosterone concentration (T-T). Various analyses related to T-T and SAF as coronary risk markers were performed.
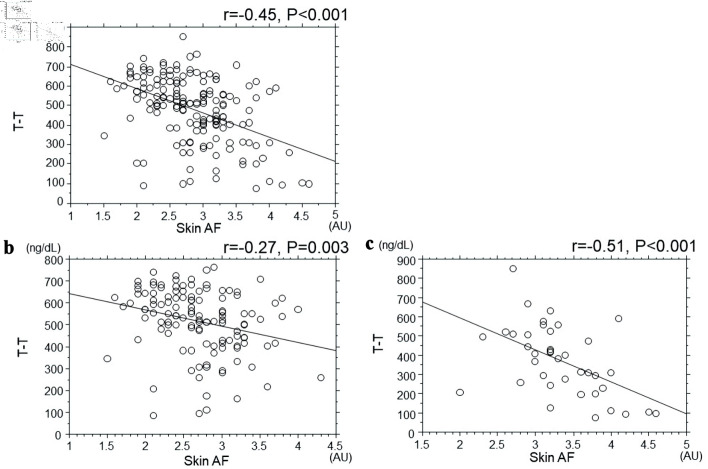
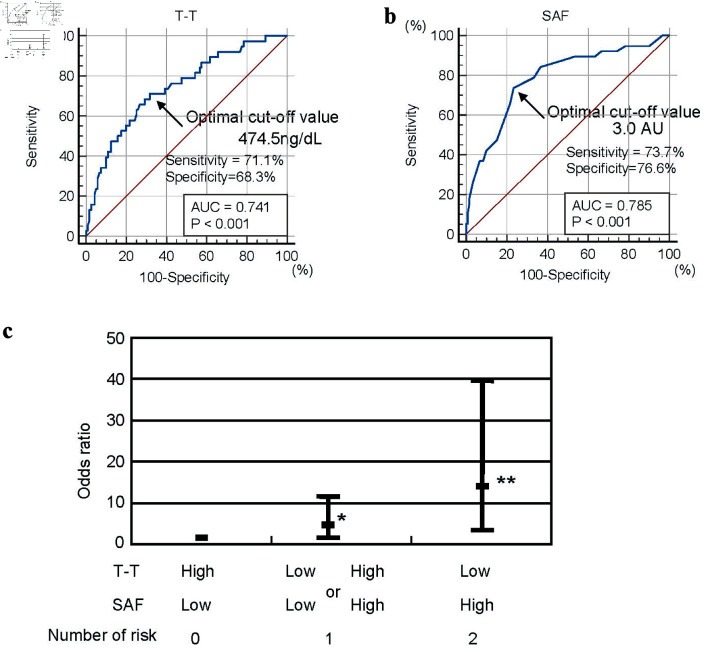
Results: T-T was significantly lower, and SAF was significantly higher in patients with CAD than in patients with non-CAD. A significant negative correlation was found between T-T and SAF (r = -0.45, P < 0.001), and the correlation was stronger in patients with CAD than in patients with non-CAD (non-CAD, r = -0.27, P = 0.003; CAD, r = -0.51, P < 0.001). However, both T-T and SAF had significant associations with triglyceride-glucose index as an insulin resistance marker and cardio-ankle vascular index as an arterial function marker. Multiple regression analysis revealed that both T-T and SAF were selected as independent variables to the presence of CAD as a dependent variable. However, the odds ratio increased due to the merger of two coronary risk markers, low T-T and high SAF (odds ratio: one risk marker: 3.24, 95% confidence interval: 1.01 - 10.50, P = 0.045; two risk markers: 13.22, 95% confidence interval: 3.41 - 39.92, P < 0.001).
Conclusions: The results of this cross-sectional study indicate that T-T and SAF are closely related in CAD patients with T2DM. It also shows that insulin resistance and arterial dysfunction are in the background of both indicators. Additionally, not only are both indicators independent coronary risk markers, but the overlap of both indicators increases their weight as coronary risk markers.
Keywords: Cardio-ankle vascular index; Coronary artery disease; Male; Skin autofluorescence; Testosterone; Triglyceride-glucose index; Type 2 diabetes mellitus.
Copyright 2024, Hitsumoto.
Conflict of interest statement
None to declare.
Figures
References
-
- Ueki K, Sasako T, Okazaki Y, Kato M, Okahata S, Katsuyama H, Haraguchi M. et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951–964. doi: 10.1016/S2213-8587(17)30327-3. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous