

The arrhythmic substrate of hypertrophic cardiomyopathy using ECG imaging
- PMID: 39206383
- PMCID: PMC11350108
- DOI: 10.3389/fphys.2024.1428709
The arrhythmic substrate of hypertrophic cardiomyopathy using ECG imaging
Abstract
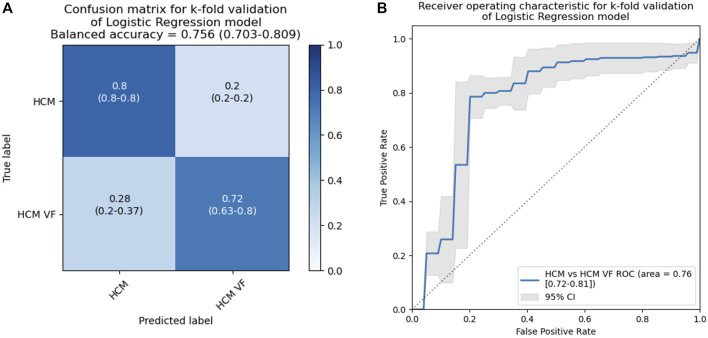
Introduction: Patients with hypertrophic cardiomyopathy (HCM) are at risk for lethal ventricular arrhythmia, but the electrophysiological substrate behind this is not well-understood. We used non-invasive electrocardiographic imaging to characterize patients with HCM, including cardiac arrest survivors. Methods: HCM patients surviving ventricular fibrillation or hemodynamically unstable ventricular tachycardia (n = 17) were compared to HCM patients without a personal history of potentially lethal arrhythmia (n = 20) and a pooled control group with structurally normal hearts. Subjects underwent exercise testing by non-invasive electrocardiographic imaging to estimate epicardial electrophysiology. Results: Visual inspection of reconstructed epicardial HCM maps revealed isolated patches of late activation time (AT), prolonged activation-recovery intervals (ARIs), as well as reversal of apico-basal trends in T-wave inversion and ARI compared to controls (p < 0.005 for all). AT and ARI were compared between groups. The pooled HCM group had longer mean AT (60.1 ms vs. 52.2 ms, p < 0.001), activation dispersion (55.2 ms vs. 48.6 ms, p = 0.026), and mean ARI (227 ms vs. 217 ms, p = 0.016) than structurally normal heart controls. HCM ventricular arrhythmia survivors could be differentiated from HCM patients without a personal history of life-threatening arrhythmia by longer mean AT (63.2 ms vs. 57.4 ms, p = 0.007), steeper activation gradients (0.45 ms/mm vs. 0.36 ms/mm, p = 0.011), and longer mean ARI (234.0 ms vs. 221.4 ms, p = 0.026). A logistic regression model including whole heart mean activation time and activation recovery interval could identify ventricular arrhythmia survivors from the HCM cohort, producing a C statistic of 0.76 (95% confidence interval 0.72-0.81), with an optimal sensitivity of 78.6% and a specificity of 79.8%. Discussion: The HCM epicardial electrotype is characterized by delayed, dispersed conduction and prolonged, dispersed activation-recovery intervals. Combination of electrophysiologic measures with logistic regression can improve differentiation over single variables. Future studies could test such models prospectively for risk stratification of sudden death due to HCM.
Keywords: electrocardiographic imaging; hypertrophic cardiomyopathy; implantable defibrillator; risk stratification; sudden death.
Copyright © 2024 Chow, Leong, Shun-Shin, Jones, Guttmann, Mohiddin, Lambiase, Elliott, Ormerod, Koa-Wing, Lefroy, Lim, Linton, Ng, Qureshi, Whinnett, Peters, Francis, Varnava and Kanagaratnam.
Conflict of interest statement
Medtronic has not influenced or sponsored any of the research here but has provided speaker fees to PK for a topic unrelated to this work. Imperial Innovations holds the patent for the intellectual property of the Ventricular Conduction Stability algorithm on behalf of the authors MS-S, KL, FN, AV, DF, and PK. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures






References
-
- Finocchiaro G., Sheikh N., Leone O., Westaby J., Mazzarotto F., Pantazis A., et al. (2021). Arrhythmogenic potential of myocardial disarray in hypertrophic cardiomyopathy: genetic basis, functional consequences and relation to sudden cardiac death. EP Eur. 23 (7), 985–995. 10.1093/europace/euaa348 - DOI - PubMed
LinkOut - more resources
Full Text Sources