

Peripheral neuropathy prevalence and effect on mobility 12 months after prosthesis prescription among individuals with dysvascular lower extremity amputation
- PMID: 39206670
- PMCID: PMC11828668
- DOI: 10.1002/pmrj.13253
Peripheral neuropathy prevalence and effect on mobility 12 months after prosthesis prescription among individuals with dysvascular lower extremity amputation
Abstract
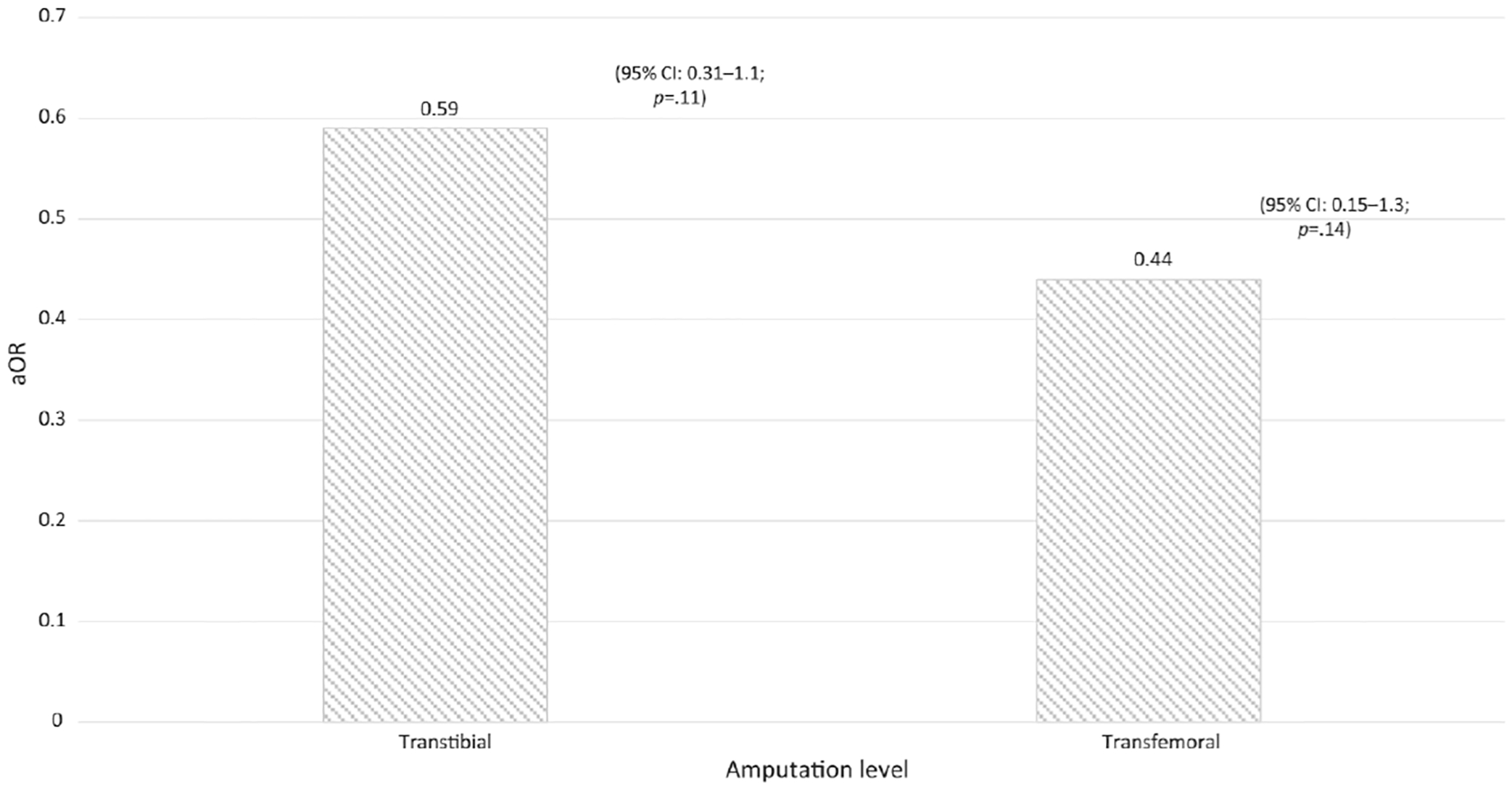
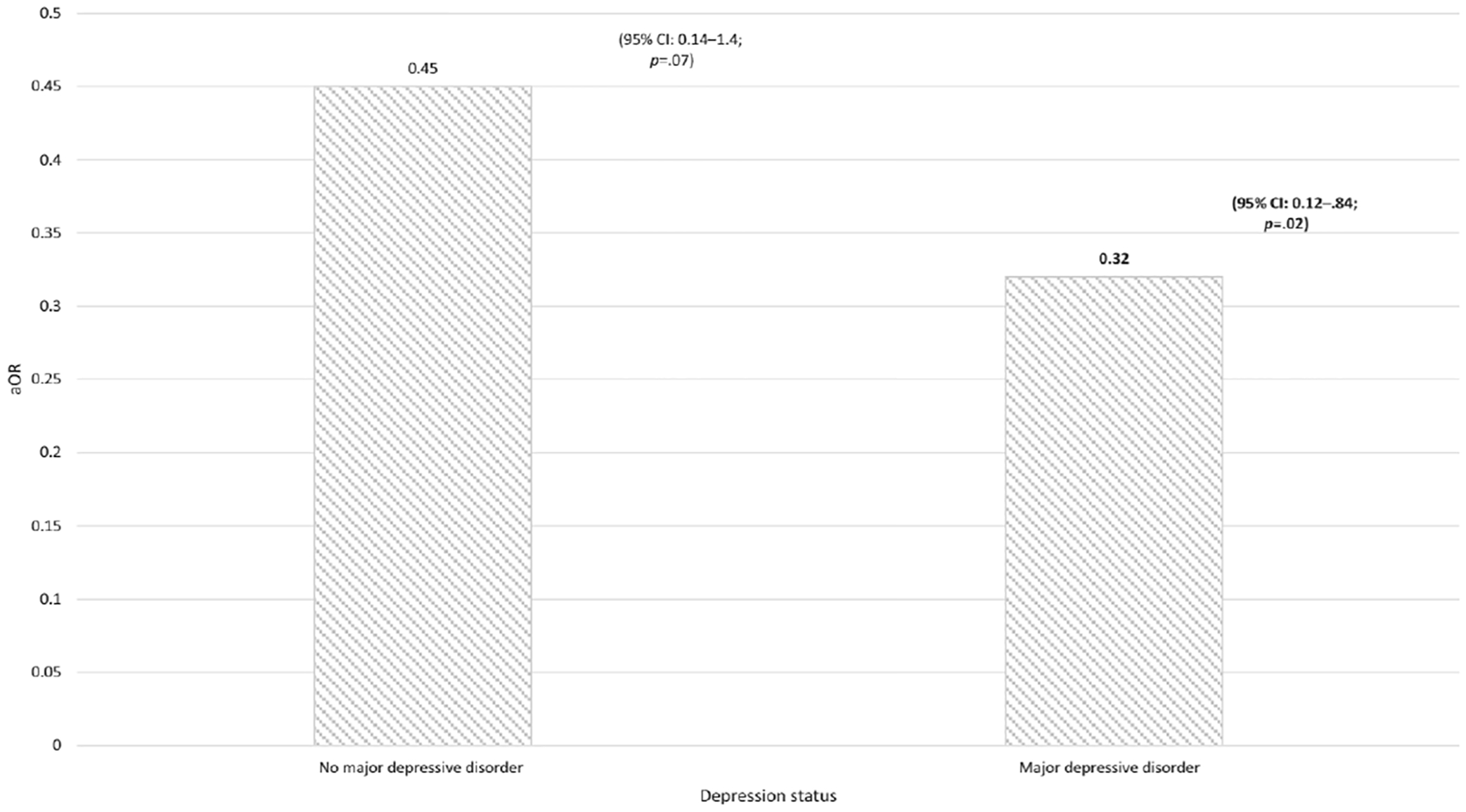
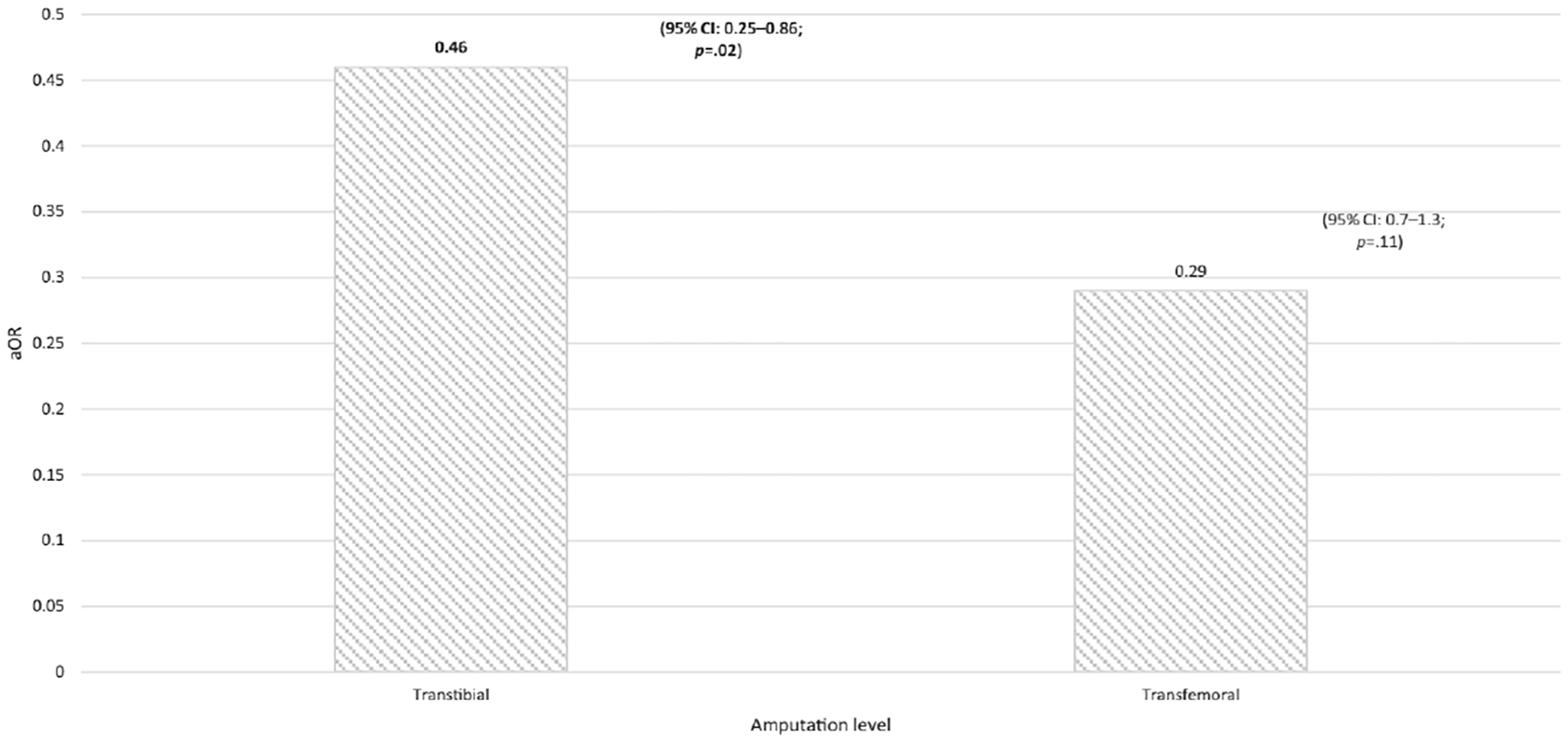
Objective: To determine the prevalence of peripheral neuropathy (PN) and its effect on mobility in patients who were prescribed a lower limb prosthesis (LLP) after an incident dysvascular transtibial (TT) or transfemoral (TF) lower extremity amputation (LEA). We also sought to determine if the effect of PN on mobility was modified by amputation level or depression.
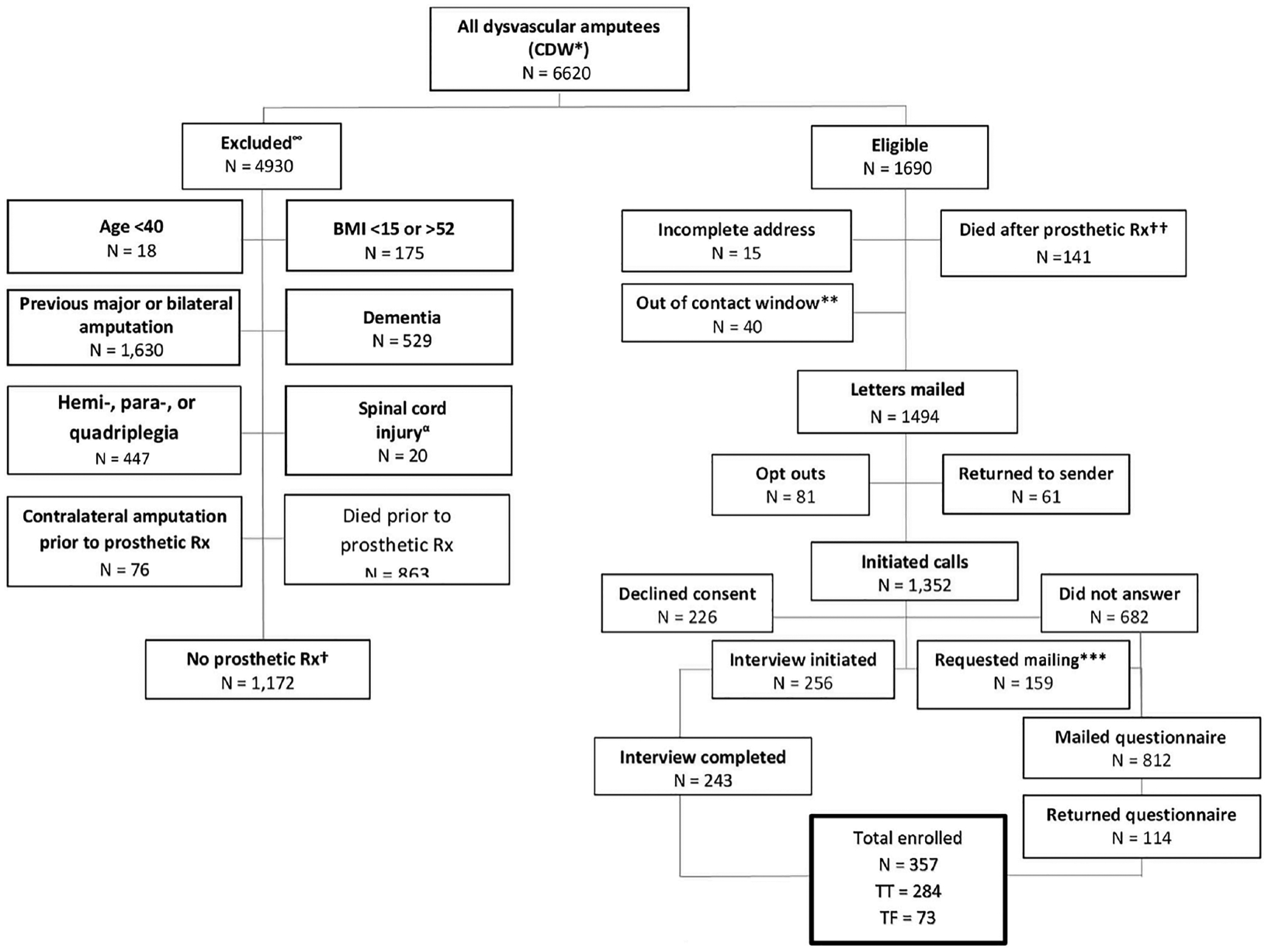
Design: Participants were identified retrospectively through the Veterans Affairs (VA) Corporate Data Warehouse (CDW) from March 1, 2018, to November 30, 2020, then were contacted prospectively to obtain their self-reported mobility. Multiple logistic regression was used to control for potential confounders and identify potential effect modifiers.
Setting: The VA CDW, the National Prosthetics Patient Database, participant mailings and phone calls.
Participants: Three hundred fifty-seven individuals who underwent a TT or TF amputation due to diabetes and/or peripheral arterial disease and were fitted with a qualifying LLP.
Interventions: Not applicable.
Main outcomes measures: The Locomotor Capabilities Index basic and advanced mobility subscale scores.
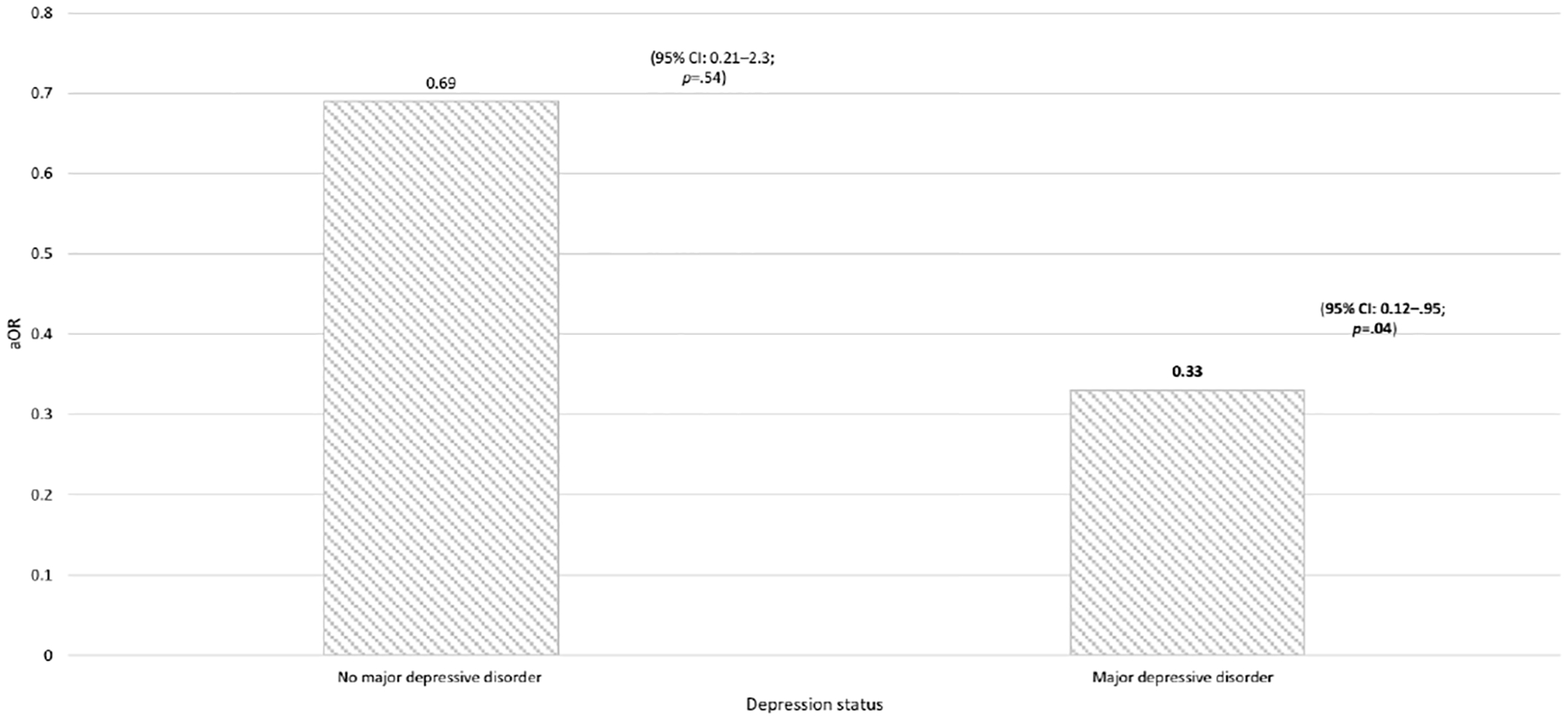
Results: Two-hundred thirty seven participants (66%) had a diagnosis of PN prior to prosthesis prescription. The detrimental effect of PN on achieving basic and advanced mobility was significant after adjusting for potential confounding factors (adjusted odds ratio [aOR], 0.53; 95% confidence interval [CI], 0.30-0.94; p = .03 and aOR, 0.43; 95% CI, 0.24-0.77; p = .005, respectively). The detrimental effect of PN was more pronounced in patients with depression, especially for advanced mobility (aOR, 0.36; 95% CI, 0.14-0.95; p = .04) versus no depression (aOR, 0.53; 95% CI, 0.27-1.0; p = .07).
Conclusions: PN is common in patients who have undergone an LEA due to diabetes and/or vascular disease and patients with this diagnosis should be carefully evaluated. Targeted rehabilitation programs to mitigate its potential detrimental effects on mobility are important and should specifically include mental health assessment and treatment.
Published 2024. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
DISCLOSURES
The authors report there are no competing interests to declare.
Figures
References
-
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008; 89(3):422–429. - PubMed
-
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3): 480–486. - PubMed
-
- Asano M, Rushton P, Miller WC, Deathe BA. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet Orthot Int. 2008;32(2):231–243. - PubMed
-
- Chen MC, Lee SS, Hsieh YL, Wu SJ, Lai CS, Lin SD. Influencing factors of outcome after lower-limb amputation: a five-year review in a plastic surgical department. Ann Plast Surg. 2008;61(3):314–318. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
