

Monitoring and modulation of respiratory drive in patients with acute hypoxemic respiratory failure in spontaneous breathing
- PMID: 39207721
- PMCID: PMC11582292
- DOI: 10.1007/s11739-024-03715-3
Monitoring and modulation of respiratory drive in patients with acute hypoxemic respiratory failure in spontaneous breathing
Abstract
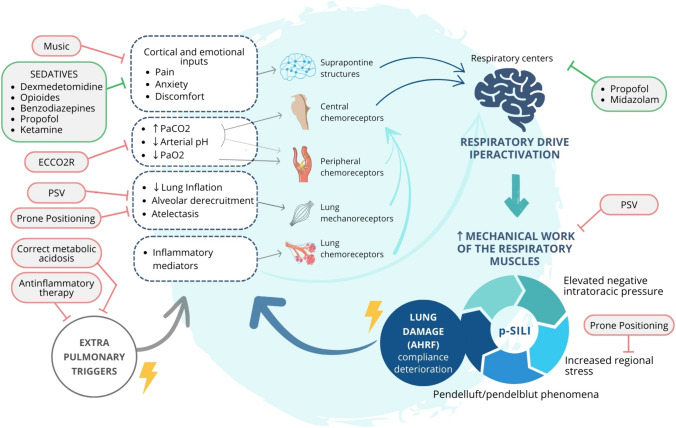
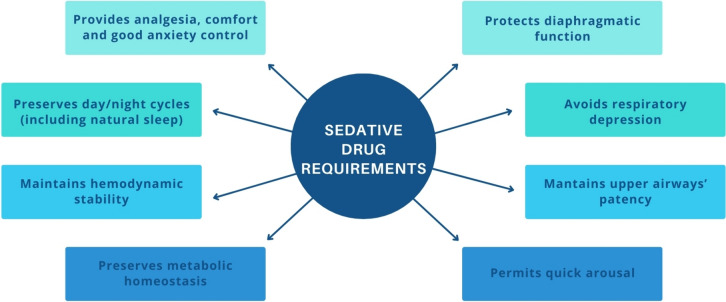
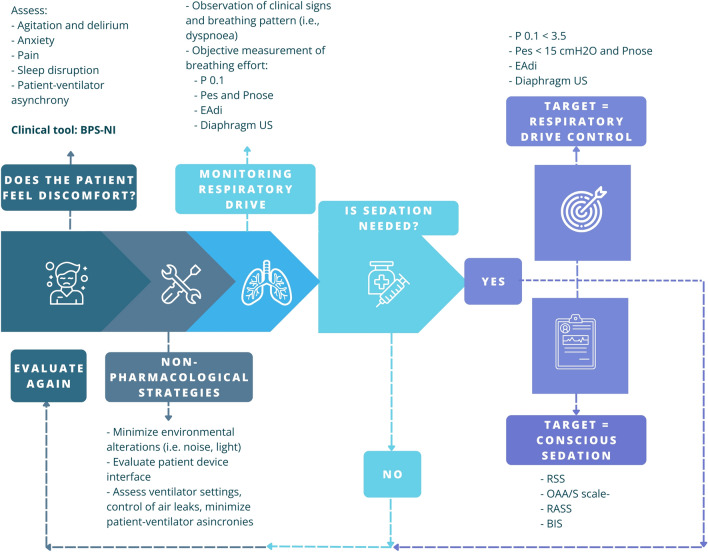
Non-invasive respiratory support, namely, non-invasive ventilation, continuous positive airway pressure, and high-flow nasal cannula, has been increasingly used worldwide to treat acute hypoxemic respiratory failure, giving the benefits of keeping spontaneous breathing preserved. In this scenario, monitoring and controlling respiratory drive could be helpful to avoid patient self-inflicted lung injury and promptly identify those patients that require an upgrade to invasive mechanical ventilation. In this review, we first describe the physiological components affecting respiratory drive to outline the risks associated with its hyperactivation. Further, we analyze and compare the leading strategies implemented for respiratory drive monitoring and discuss the sedative drugs and the non-pharmacological approaches used to modulate respiratory drive during non-invasive respiratory support. Refining the available techniques and rethinking our therapeutic and monitoring targets can help critical care physicians develop a personalized and minimally invasive approach.
Keywords: Acute hypoxemic respiratory failure; Monitoring; Non-invasive respiratory support; Respiratory drive; Sedation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: RT, RF, LT, IC, AMarchioni, and EC declare patent N. 102021000007478 “APPARATO PER IL RILEVAMENTO ED IL MONITORAGGIO DELLA PRESSIONE NASALE” released on March 28th 2023 by the Italian Ministry of Enterprises and Made in Italy. RT, RF, LT, AMarchioni, and EC are co-founders of IREC ltd (VAT 02959080355) (Reggio Emilia, Italy). RT received travel support and fees from GSK, SEDA, Guidotti, United HealthCare Services. AMocellin, FG, SR, MT, AP, GB, JM, and DP have no competing interests with any organization or entity with a financial interest in competition with the subject, matter, or materials discussed in this manuscript.
Figures
References
-
- Oczkowski S, Ergan B, Bos L et al (2022) ERS clinical practice guidelines: high-flow nasal cannula in acute respiratory failure. Eur Respir J 59(4):2101574 - PubMed
-
- Qvist J, Pontoppidan H, Wilson RS et al (1975) Hemodynamic responses to mechanical ventilation with PEEP: the effect of hypervolemia. Anesthesiology 42(1):45–55 - PubMed
-
- Bellani G, Laffey JG, Pham T et al (2017) Noninvasive ventilation of patients with acute respiratory distress syndrome. Insights from the LUNG SAFE study. Am J Respir Crit Care Med 195(1):67–77 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
