

Electronic Health Record Usability, Satisfaction, and Burnout for Family Physicians
- PMID: 39207759
- PMCID: PMC11362862
- DOI: 10.1001/jamanetworkopen.2024.26956
Electronic Health Record Usability, Satisfaction, and Burnout for Family Physicians
Abstract
Importance: Electronic health record (EHR) work has been associated with decreased physician well-being. Understanding the association between EHR usability and physician satisfaction and burnout, and whether team and technology strategies moderate this association, is critical to informing efforts to address EHR-associated physician burnout.
Objectives: To measure family physician satisfaction with their EHR and EHR usability across functions and evaluate the association of EHR usability with satisfaction and burnout, as well as the moderating association of 4 team and technology EHR efficiency strategies.
Design, setting, and participants: This study uses data from a cross-sectional survey conducted from December 12, 2021, to October 17, 2022, of all family physicians seeking American Board of Family Medicine recertification in 2022.
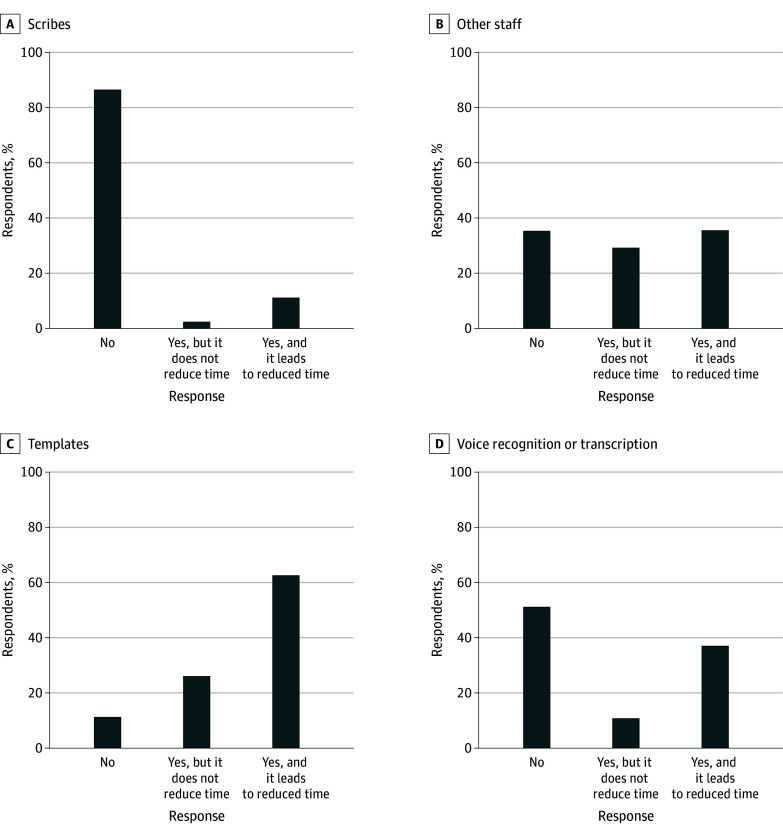
Exposure: Physicians perceived EHR usability across 6 domains, as well as adoption of 4 EHR efficiency strategies: scribes, support from other staff, templated text, and voice recognition or transcription.
Main outcomes and measures: Physician EHR satisfaction and frequency of experiencing burnout measured with a single survey item ("I feel burned out from my work"), with answers ranging from "never" to "every day."
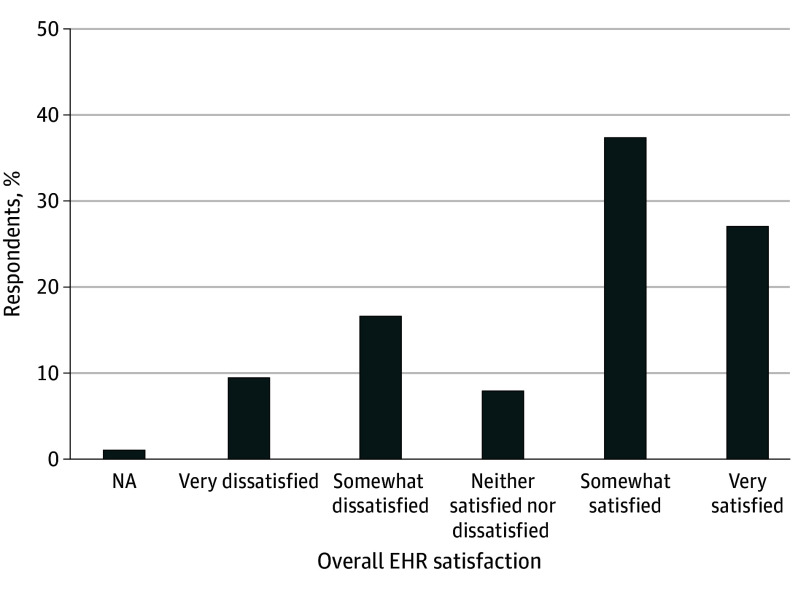
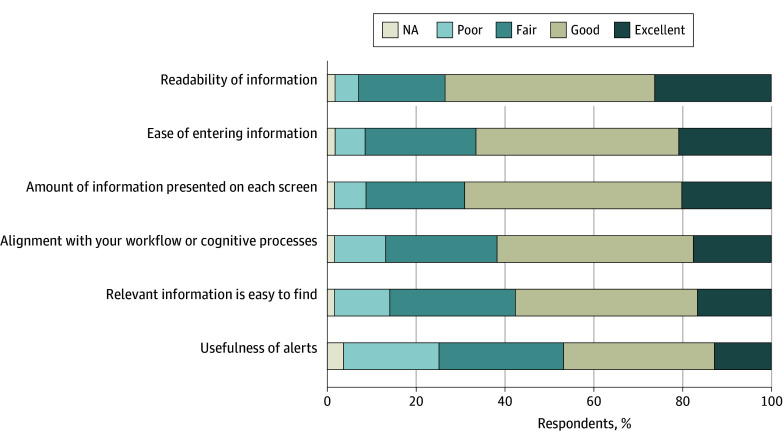
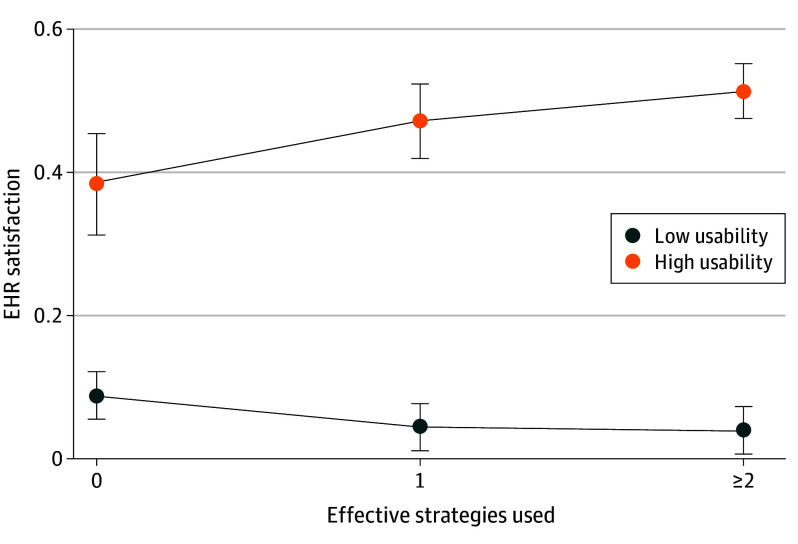
Results: Of the 2067 physicians (1246 [60.3%] younger than 50 years; 1051 men [50.9%]; and 1729 [86.0%] practicing in an urban area) who responded to the survey, 562 (27.2%) were very satisfied and 775 (37.5%) were somewhat satisfied, while 346 (16.7%) were somewhat dissatisfied and 198 (9.6%) were very dissatisfied with their EHR. Readability of information had the highest usability, with 543 physicians (26.3%) rating it as excellent, while usefulness of alerts had the lowest usability, with 262 physicians (12.7%) rating it as excellent. In multivariable models, good or excellent usability for entering data (β = 0.09 [95% CI, 0.05-0.14]; P < .001), alignment with workflow processes (β = 0.11 [95% CI, 0.06-0.16]; P < .001), ease of finding information (β = 0.14 [95% CI, 0.09-0.19]; P < .001), and usefulness of alerts (β = 0.11 [95% CI, 0.06-0.16]; P < .001) were associated with physicians being very satisfied with their EHR. In addition, being very satisfied with the EHR was associated with reduced frequency of burnout (β = -0.64 [95% CI, -1.06 to -0.22]; P < .001). In moderation analysis, only physicians with highly usable EHRs saw improvements in satisfaction from adopting efficiency strategies.
Conclusions and relevance: In this survey study of physician EHR usability and satisfaction, approximately one-fourth of family physicians reported being very satisfied with their EHR, while another one-fourth reported being somewhat or very dissatisfied, a concerning finding amplified by the inverse association between EHR satisfaction and burnout. Electronic health record-based alerts had the lowest reported usability, suggesting EHR vendors should focus their efforts on improving alerts. Electronic health record efficiency strategies were broadly adopted, but only physicians with highly usable EHRs realized gains in EHR satisfaction from using these strategies, suggesting that EHR burden-reduction interventions are likely to have heterogenous associations across physicians with different EHRs.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
