

Pulmonary hypertension associated with lung diseases
- PMID: 39209469
- PMCID: PMC11525344
- DOI: 10.1183/13993003.01200-2024
Pulmonary hypertension associated with lung diseases
Abstract
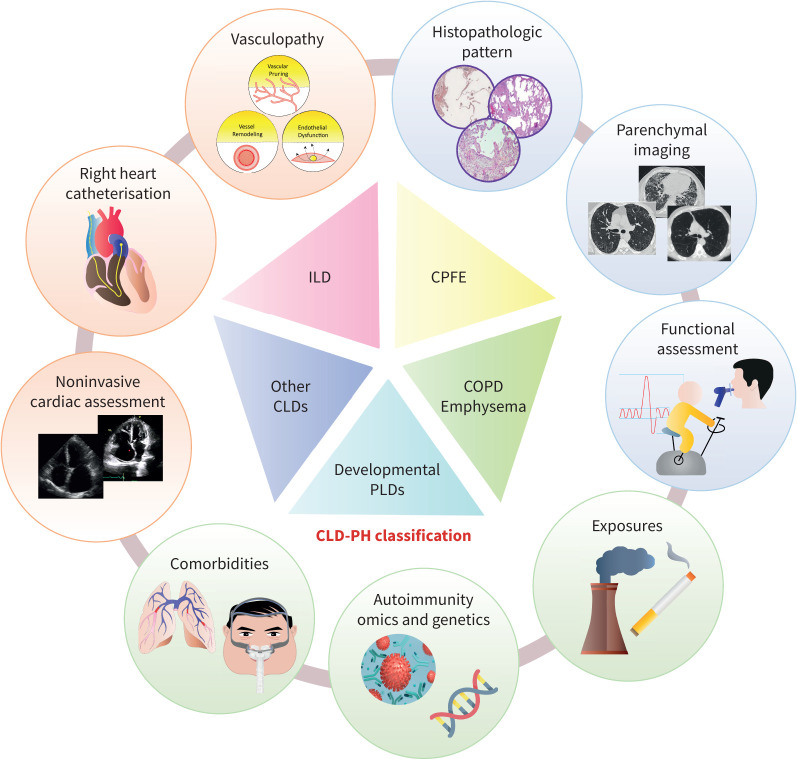
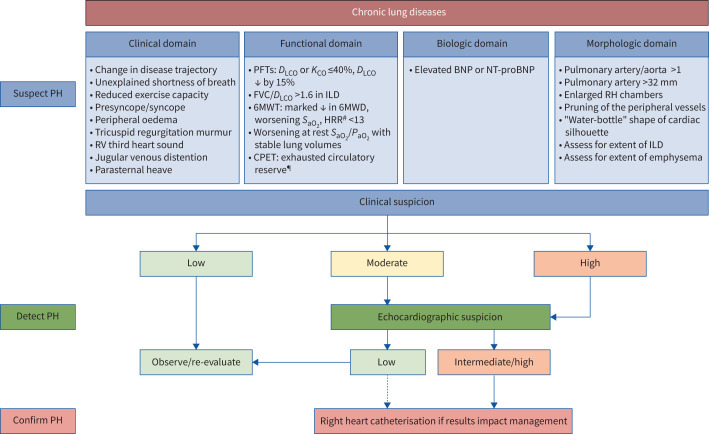
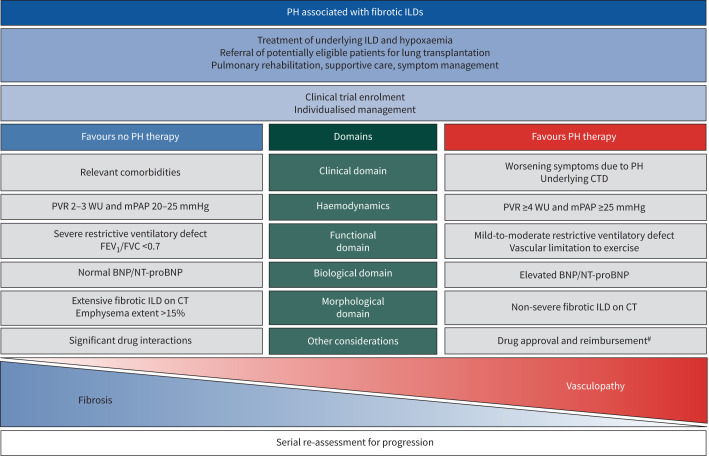
Pulmonary hypertension (PH) associated with chronic lung disease (CLD) is both common and underrecognised. The presence of PH in the setting of lung disease has been consistently shown to be associated with worse outcomes. Recent epidemiological studies have advanced understanding of the heterogeneity of this patient population and shown that defining both the specific type of CLD as well as the severity of PH (i.e. deeper phenotyping) is necessary to inform natural history and prognosis. A systematic diagnostic approach to screening and confirmation of suspected PH in CLD is recommended. Numerous uncontrolled studies and one phase 3 randomised, controlled trial have suggested a benefit in treating PH in some patients with CLD, specifically those with fibrotic interstitial lung disease (ILD). However, other studies in diseases such as COPD-PH showed adverse outcomes with some therapies. Given the expanding list of approved pharmacological treatments for pulmonary arterial hypertension, developing a treatment algorithm for specific phenotypes of CLD-PH is required. This article will summarise existing data in COPD, ILD and other chronic lung diseases, and provide recommendations for classification of CLD-PH and approach to the diagnosis and management of these challenging patients.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: O.A. Shlobin reports consultancy fees from United Therapeutics, Merck, Janssen and Aerami, payment or honoraria for lectures, presentations, manuscript writing or educational events from Ferrera and United Therapeutics, participation on a data safety monitoring board or advisory board with Janssen, and leadership roles with ACCP/Chest and World Symposium on Pulmonary Hypertension task force. Y. Adir reports consultancy fees and payment or honoraria for lectures, presentations, manuscript writing or educational events from MSD Israel and Bayer Israel, support for attending meetings from BI Israel and RAFA Israel, and participation on a data safety monitoring board or advisory board with MSD, GB and Acceleron. J.A. Barbera reports grants from Merck Sharp & Dome and Ferrer International, consultancy fees from Merck Sharp & Dome, Janssen-Cilag and Ferrer International, payment or honoraria for lectures, presentations, manuscript writing or educational events from Merck Sharp & Dome, Janssen-Cilag, Ferrer International and AOP Orphan, support for attending meetings from Merck Sharp & Dome and Janssen-Cilag, and a leadership role with the World Symposium on Pulmonary Hypertension task force. V. Cottin reports consultancy fees and payment or honoraria for lectures, presentations, or educational events from Ferrer/United Therapeutics. S. Harari reports consultancy fees from Roche-Boehringer Ingelheim, payment or honoraria for lectures, presentations, manuscript writing or educational events from Boehringer Ingelheim, participation on a data safety monitoring board or advisory board “Prise en charge pragmatique de la fibrose pulmonaire idiopathique en progression: essai randomisé PROGRESSION-IPF”, and leadership roles with the World Symposium on Pulmonary Hypertension task force, FERS of the ERS and officer of the society, and FATS of the ATS. E-M. Jutant reports consultancy fees from Chiesi, payment or honoraria for lectures, presentations, manuscript writing or educational events from Chiesi, GSK, MSD and AstraZeneca, support for attending meetings from Janssen and MSD, and a leadership role with the World Symposium on Pulmonary Hypertension task force. J. Pepke-Zaba reports grants from MSD, consultancy fees from MSD, Janssen, Gossamer and Ferrer, support for attending meetings from Janssen, and a leadership role with the World Symposium on Pulmonary Hypertension task force. H-A. Ghofrani reports consultancy fees from Gossamer Bio, Inc., Aerovate, Altavant, Bayer AG, Attgeno, Janssen/Actelion, MSD/Acceleron, Pfizer, Liquidia, Morphic and Keros, payment or honoraria for lectures, presentations, manuscript writing or educational events from Bayer AG, Janssen/Actelion, Gossamer Bio, Keros and MSD/Acceleron, participation on a data safety monitoring board or advisory board with Aerovate, Altavant, Attgeno, Janssen/Actelion, Insmed, MSD/Acceleron, Pfizer and Bayer AG, and the following financial (or non-financial) interests: the author's spouse is and employee of Liquidia. R. Channick reports consultancy fees from Bayer, Merck, Gossamer, Respira and Janssen, payment or honoraria for lectures, presentations, manuscript writing or educational events from Bayer and Janssen, and participation on a data safety monitoring board or advisory board with Altavant.
Figures
Comment in
-
The Seventh World Symposium on Pulmonary Hypertension: our journey to Barcelona.Eur Respir J. 2024 Oct 31;64(4):2401222. doi: 10.1183/13993003.01222-2024. Print 2024 Oct. Eur Respir J. 2024. PMID: 39209470 Free PMC article.