

Pathology and pathobiology of pulmonary hypertension: current insights and future directions
- PMID: 39209474
- PMCID: PMC11533988
- DOI: 10.1183/13993003.01095-2024
Pathology and pathobiology of pulmonary hypertension: current insights and future directions
Abstract
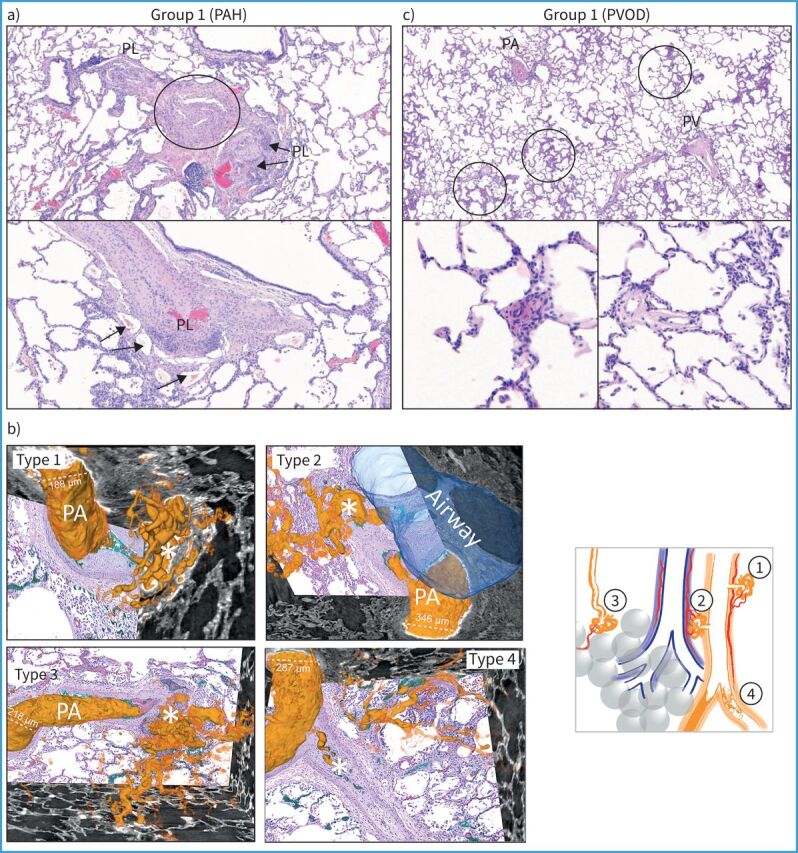
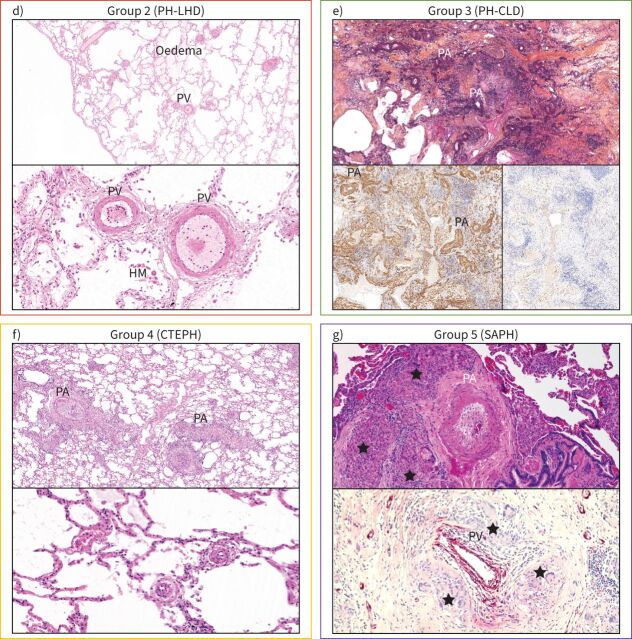
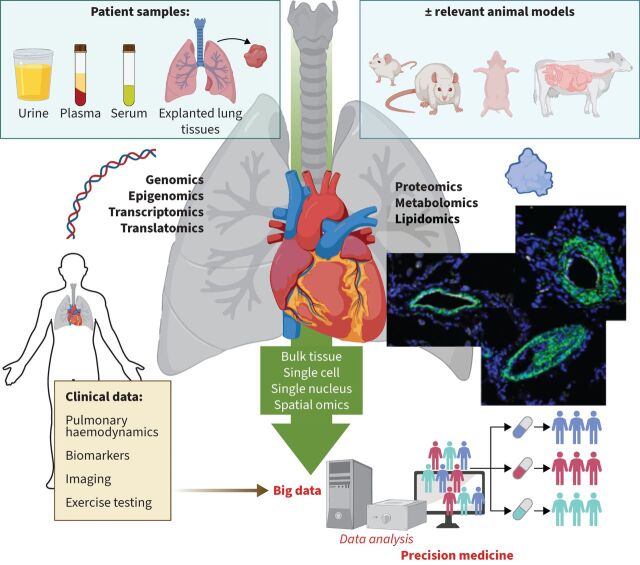
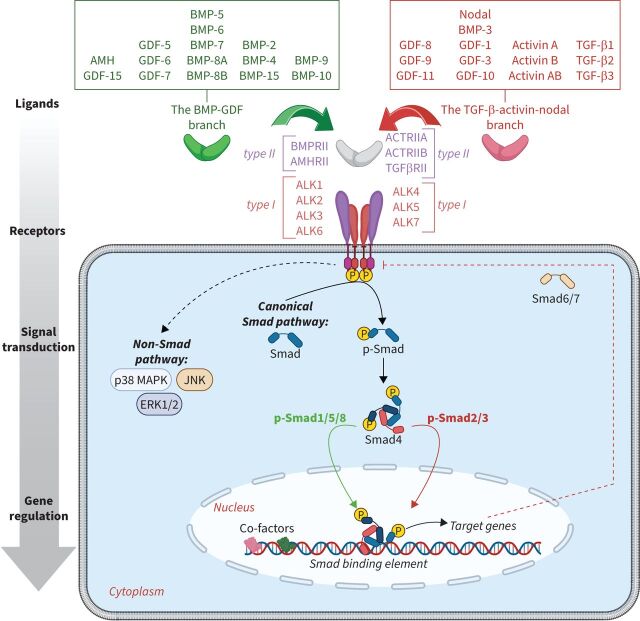
In recent years, major advances have been made in the understanding of the cellular and molecular mechanisms driving pulmonary vascular remodelling in various forms of pulmonary hypertension, including pulmonary arterial hypertension, pulmonary hypertension associated with left heart disease, pulmonary hypertension associated with chronic lung disease and hypoxia, and chronic thromboembolic pulmonary hypertension. However, the survival rates for these different forms of pulmonary hypertension remain unsatisfactory, underscoring the crucial need to more effectively translate innovative scientific knowledge into healthcare interventions. In these proceedings of the 7th World Symposium on Pulmonary Hypertension, we delve into recent developments in the field of pathology and pathophysiology, prioritising them while questioning their relevance to different subsets of pulmonary hypertension. In addition, we explore how the latest omics and other technological advances can help us better and more rapidly understand the myriad basic mechanisms contributing to the initiation and progression of pulmonary vascular remodelling. Finally, we discuss strategies aimed at improving patient care, optimising drug development, and providing essential support to advance research in this field.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: C. Guignabert reports grants from Acceleron Pharma, MSD, Corteria Pharmaceuticals, Structure Therapeutics (ex-ShouTi) and Gossamer Bio, payment or honoraria for lectures, presentations, manuscript writing or educational events from MSD, and patents planned, issued or pending (WO/2024/023139, WO/2018/011376). J. Aman has no potential conflicts of interest to disclose. S. Bonnet reports grants from Morphic Therapeutic, Sunshine Bio and Janssen, consultancy fees from Morphic Therapeutic and Chiesi, and participation on a data safety monitoring board or advisory board with Morphic Therapeutic and Allienaire. P. Dorfmüller reports payment or honoraria for lectures, presentations, manuscript writing or educational events from AstraZeneca. A.J. Olschewski reports grants from Austrian Science Fund (FWF) (10.55776/I6299 and 10.55776/KLI1153), payment or honoraria for lectures, presentations, manuscript writing or educational events from MSD, patents pending (PCT/EP2017/055440), and stock (or stock options) with Bayer. S. Pullamsetti reports grants and consultancy fees from Gossamer Bio. M. Rabinovitch reports consultancy fees from Pfizer, Amgen, Merck and Tiakis, payment or honoraria for lectures, presentations, manuscript writing or educational events from NIH, patents planned, issued or pending (FK506: tacrolimus in pulmonary hypertension), participation on a data safety monitoring board or advisory board with Amgen and NIH, is associate editor for JACC BTS, receipt of equipment, materials, drugs, medical writing, gifts or other services from Tiakis (tiprelestat). R.T. Schermuly reports grants from Chiesi and Attgeno, and consultancy fees from Gossamer, Attgeno and Chiesi. M. Humbert reports grants from Gossamer and Merck, consultancy fees from 35 Pharma, Aerovate, AOP Orphan, Chiesi, Ferrer, Gossamer, Janssen, Keros, Liquidia, Merck, Novartis, Respira, Roivant and United Therapeutics, payment or honoraria for lectures, presentations, manuscript writing or educational events from Janssen and Merck, and participation on a data safety monitoring board or advisory board with 35 Pharma, Aerovate, Janssen, Keros, Merck, Novartis and United Therapeutics. K.R. Stenmark reports grants from NIH/NHLBI and DoD, and a leadership role with PVRI.
Figures
Comment in
-
The Seventh World Symposium on Pulmonary Hypertension: our journey to Barcelona.Eur Respir J. 2024 Oct 31;64(4):2401222. doi: 10.1183/13993003.01222-2024. Print 2024 Oct. Eur Respir J. 2024. PMID: 39209470 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical