

Pulmonary hypertension associated with left heart disease
- PMID: 39209478
- PMCID: PMC11525340
- DOI: 10.1183/13993003.01344-2024
Pulmonary hypertension associated with left heart disease
Abstract
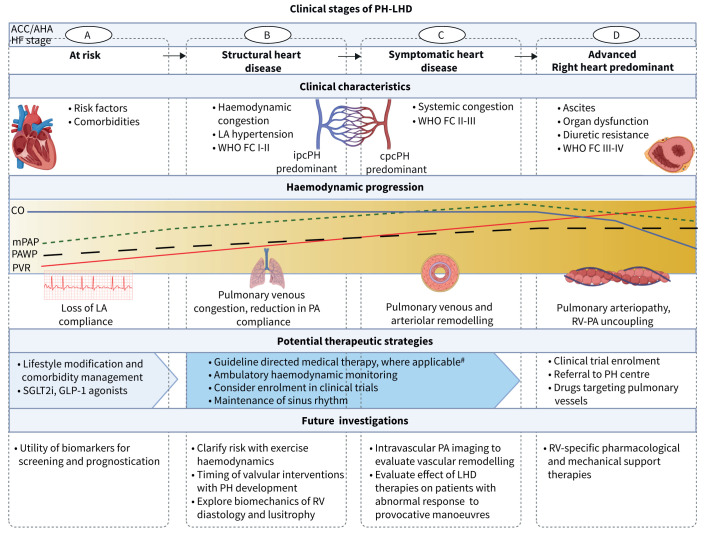
Left heart disease (LHD) is the most common cause of pulmonary hypertension (PH), which may be classified further as isolated post-capillary (ipcPH) or combined post- and pre-capillary PH (cpcPH). The 7th World Symposium on Pulmonary Hypertension PH-LHD task force reviewed newly reported randomised clinical trials and contemplated novel opportunities for improving outcome. Results from major randomised clinical trials reinforced prior recommendations against the use of pulmonary arterial hypertension therapy in PH-LHD outside of clinical trials, and suggested possible harm. Greater focus on phenotyping was viewed as one general strategy by which to ultimately improve clinical outcomes. This is potentially achievable by individualising ipcPH versus cpcPH diagnosis for patients with pulmonary arterial wedge pressure within a diagnostic grey zone (12-18 mmHg), and through a newly developed PH-LHD staging system. In this model, PH accompanies LHD across four stages (A=at risk, B=structural heart disease, C=symptomatic heart disease, D=advanced), with each stage characterised by progression in clinical characteristics, haemodynamics and potential therapeutic strategies. Along these lines, the task force proposed disaggregating PH-LHD to emphasise specific subtypes for which PH prevalence, pathophysiology and treatment are unique. This includes re-interpreting mitral and aortic valve stenosis through a contemporary lens, and focusing on PH within the hypertrophic cardiomyopathy and amyloid cardiomyopathy clinical spectra. Furthermore, appreciating LHD in the profile of PH patients with chronic lung disease and chronic thromboembolic pulmonary disease is essential. However, engaging LHD patients in clinical research more broadly is likely to require novel methodologies such as pragmatic trials and may benefit from next-generation analytics to interpret results.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: B.A. Maron reports grants from NIH/NHLBI and Deerfield Company, consultancy fees from Actelion and Tenax Therapeutics, and the following unlicensed patents: PCT/US2019/059890, #9,605,047 and PCT/US2020/066886. G. Bortman reports payment or honoraria for lectures, presentations, manuscript writing or educational events from Bago, Tuteur, Raffo, Aerovate, Novartis, United, Biosidus, Sandoz, Glaxo, Gador and MKD, support for attending meetings from Tuteur, Bago, Biosidus, Raffo, Sandoz, Boehringer, Gador, Glaxo and MKD, participation on a data safety monitoring board or advisory board with Aerovate and MKD, and is a member of the Argentina Heart Society, Argentina Transplant Society and LHL. T. De Marco reports grants from CareDx and Acceleron Pharm, consultancy fees from Aerovate, Boston Scientific, Atara, Kamada, Kerios, Merck, Natera, Pulnovo, Tectonic and United Therapeutics, payment or honoraria for lectures, presentations, manuscript writing or educational events from Simply Speaking PAH CME lecture, support for attending meetings from CareDx, Atara, Kamada and United Therapeutics, and participation on a data safety monitoring board or advisory board with Merck, Keros Therapeutics, Tectonic and BIAL. J.H. Huston has no potential conflicts of interest to disclose. I.M. Lang reports grants from AOP-Health, consultancy fees from Pulnovo, Janssen, MSD, Novo Norrdisk, Daiichi and Amarin, payment or honoraria for lectures, presentations, manuscript writing or educational events from MSD, Sanofi, Janssen and Daiichi, and support for attending meetings from Medtronic. S.H. Rosenkranz reports grants from Actelion, AstraZeneca, Bayer, Janssen, Lempo and MSD, consultancy fees from Abbott, Acceleron, Actelion, Aerovate, Altavant, AOP, AstraZeneca, Bayer, Ferrer, Gossamer, Janssen, Liquidia, MSD and UT, support for attending meetings from Bayer, participation on a data safety monitoring board or advisory board with Acceleron, Actelion, Aerovate, Altavant, AOP, Gossamer, Janssen, Liquidia, MSD and UT, and was ESC task force chair for the 2022 ESC/ERS guidelines on pulmonary hypertension. J-L. Vachiery reports consultancy fees from Merck, payment or honoraria for lectures, presentations, manuscript writing or educational events from Janssen, Merck, Boehringer Ingelheim and Novartis, support for attending meetings from Merck, participation on a data safety monitoring board or advisory board with Moderna, and has leadership roles with ISHLT and ESC. R.J. Tedford reports consultancy fees from Abbott, Acorai, Aria CV Inc., Acceleron/Merck, Alleviant, Boston Scientific, Cytokinetics, Edwards LifeSciences, Endotronix, Gradient, Medtronic, Morphic Therapeutics, Restore Medical and United Therapeutics, support for attending meetings from Abiomed, participation on a data safety monitoring board or advisory board with Restore Medical, stock (or stock options) with Aria CV, and is deputy editor for JHLT, and co-chair of the PH-LHD task force for WSPH.
Figures
Comment in
-
The Seventh World Symposium on Pulmonary Hypertension: our journey to Barcelona.Eur Respir J. 2024 Oct 31;64(4):2401222. doi: 10.1183/13993003.01222-2024. Print 2024 Oct. Eur Respir J. 2024. PMID: 39209470 Free PMC article.
References
-
- Brittain EL, Thenappan T, Huston JH, et al. Elucidating the clinical implications and pathophysiology of pulmonary hypertension in heart failure with preserved ejection fraction: a call to action: A science advisory from the American Heart Association. Circulation 2022; 146: e73–e88. doi: 10.1161/CIR.0000000000001079 - DOI - PMC - PubMed
-
- Alushi B, Beckhoff F, Leistner D, et al. Pulmonary hypertension in patients with severe aortic stenosis: prognostic impact after transaortic valve replacement: pulmonary hypertension in patients undergoing TAVR. JACC Cardiovasc Imaging 2019; 12: 591–601. doi: 10.1016/j.jcmg.2018.02.015 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical