

Pathophysiology of the right ventricle and its pulmonary vascular interaction
- PMID: 39209482
- PMCID: PMC11525331
- DOI: 10.1183/13993003.01321-2024
Pathophysiology of the right ventricle and its pulmonary vascular interaction
Abstract
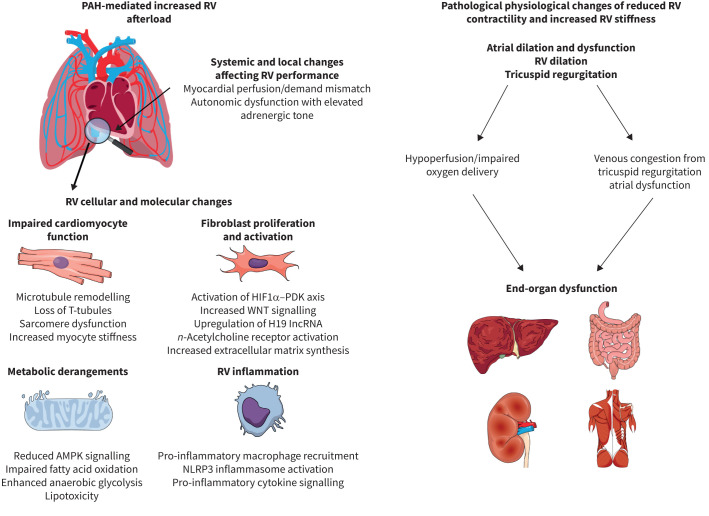
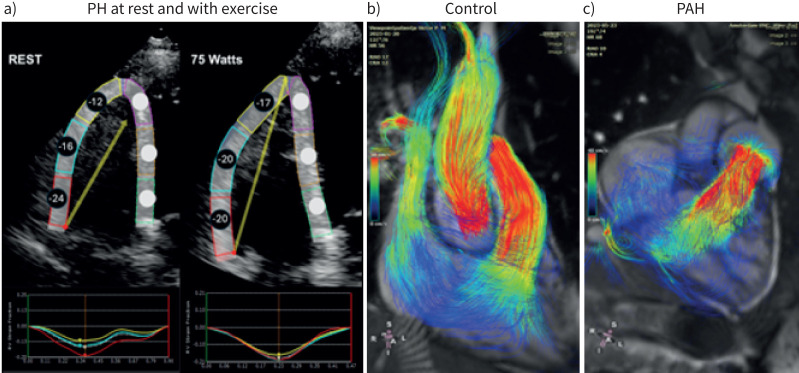
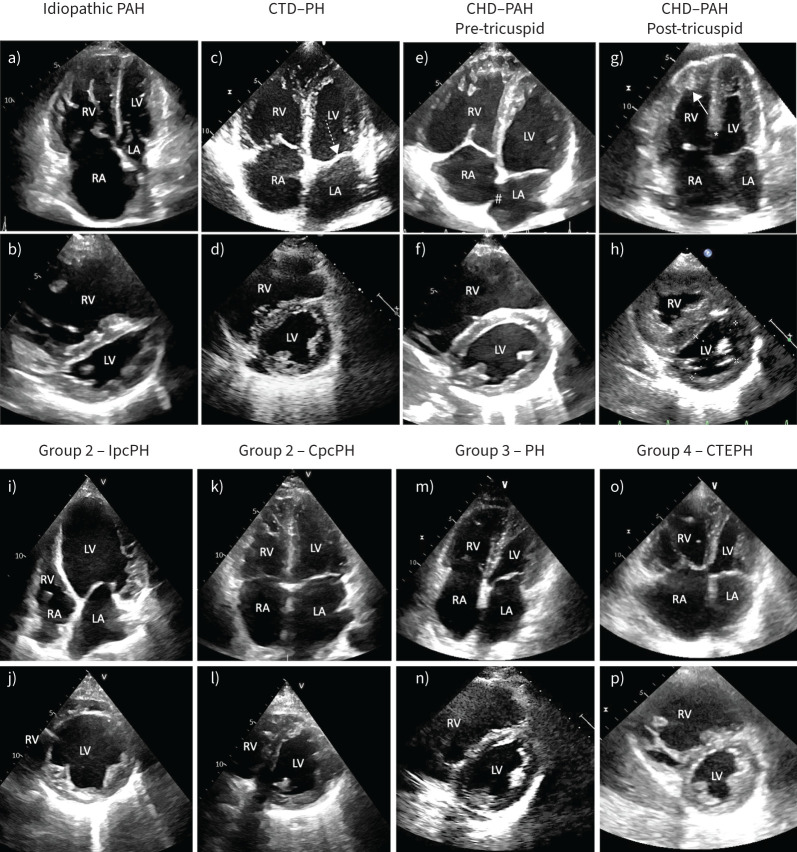
The right ventricle and its stress response is perhaps the most important arbiter of survival in patients with pulmonary hypertension of many causes. The physiology of the cardiopulmonary unit and definition of right heart failure proposed in the 2018 World Symposium on Pulmonary Hypertension have proven useful constructs in subsequent years. Here, we review updated knowledge of basic mechanisms that drive right ventricular function in health and disease, and which may be useful for therapeutic intervention in the future. We further contextualise new knowledge on assessment of right ventricular function with a focus on metrics readily available to clinicians and updated understanding of the roles of the right atrium and tricuspid regurgitation. Typical right ventricular phenotypes in relevant forms of pulmonary vascular disease are reviewed and recent studies of pharmacological interventions on chronic right ventricular failure are discussed. Finally, unanswered questions and future directions are proposed.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: A.R. Hemnes reports grants from NIH/NHLBI, consultancy fees from Bayer, Gossamer Bio, Merck, Janssen, United Therapeutics and Tenax, participation on a data safety monitoring board or advisory board with NIH/NHLBI, leadership roles with Nashville Ballet and Pulmonary Vascular Research Institute, and stock (or stock options) with Tenax Therapeutics. D.S. Celermajer has no potential conflicts of interest to disclose. M. D'Alto reports consultancy fees and payment or honoraria for lectures, presentations, manuscript writing or educational events from Merck Sharp and Dhome, Dompé, AOP and Janssen, and support for attending meetings from Dompé, AOP and Janssen. F. Haddad reports grants from Johnson & Johnson, and consultancy fees from Merck. P.M. Hassoun reports grants from NIH/NHLBI (R01 R01HL114910), and participation on a data safety monitoring board or advisory board with MSD and ARIA-CV. K.W. Prins reports grants from NHLBI (R01 HL158795 and 162927) and Bayer (PHAB grant), and consultancy fees from Edwards. R. Naeije reports consultancy fees from AOP Orphan Pharma, Johnson & Johnson, United Therapeutics and Lung Biotechnology, payment or honoraria for lectures, presentations, manuscript writing or educational events from AOP Orphan Pharma, support for attending meetings from AOP Orphan Pharma, and participation on a data safety monitoring board or advisory board with Johnson & Johnson, AOP Orphan Pharma and United Therapeutics. A. Vonk Noordegraaf reports payment or honoraria for lectures, presentations, manuscript writing or educational events from Actelion and Johnson & Johnson.
Figures
Comment in
-
The Seventh World Symposium on Pulmonary Hypertension: our journey to Barcelona.Eur Respir J. 2024 Oct 31;64(4):2401222. doi: 10.1183/13993003.01222-2024. Print 2024 Oct. Eur Respir J. 2024. PMID: 39209470 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical