

Embracing the challenges of neonatal and paediatric pulmonary hypertension
- PMID: 39209483
- PMCID: PMC11525338
- DOI: 10.1183/13993003.01345-2024
Embracing the challenges of neonatal and paediatric pulmonary hypertension
Abstract
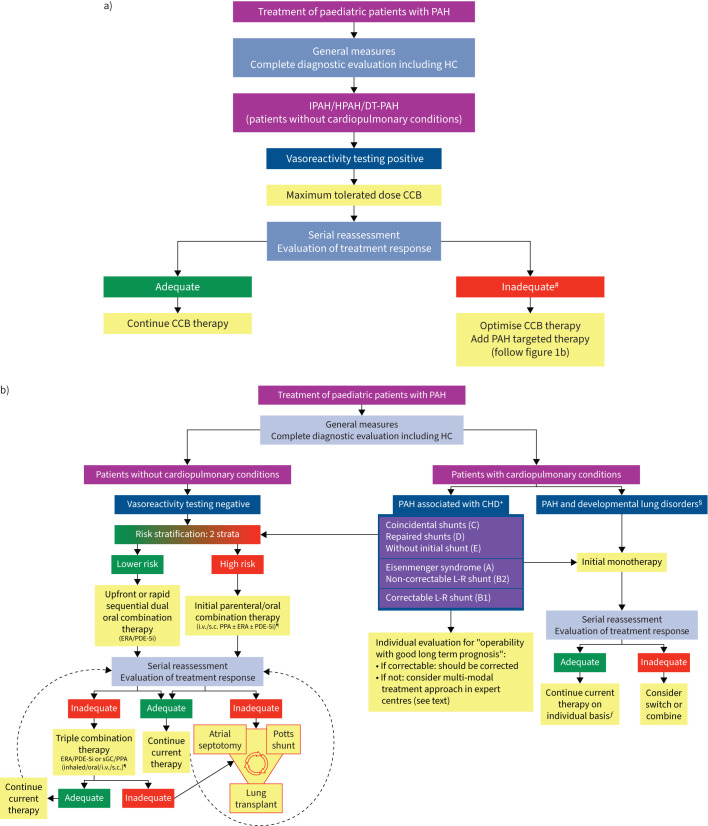
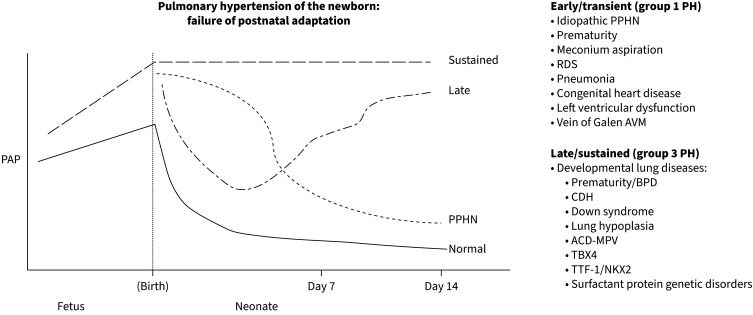
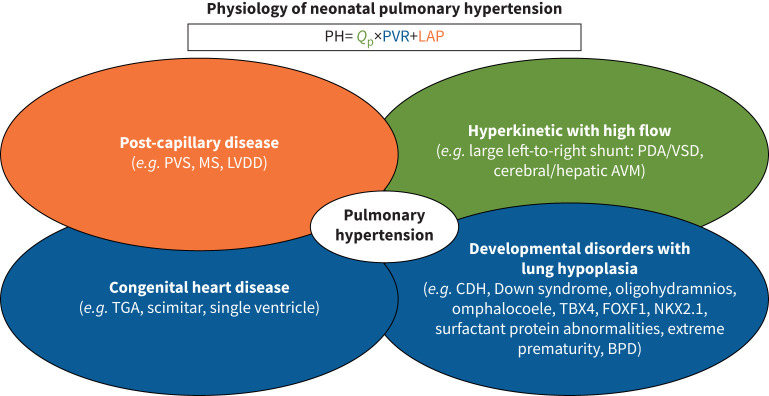
Paediatric pulmonary arterial hypertension (PAH) shares common features with adult disease, but is associated with several additional disorders and challenges that require unique approaches. This article discusses recent advances, ongoing challenges and distinct approaches for caring for infants and children with PAH, as presented by the paediatric task force of the 7th World Symposium on Pulmonary Hypertension. We provide updates on diagnosing, classifying, risk-stratifying and treating paediatric pulmonary hypertension (PH) and identify critical knowledge gaps. An updated risk stratification tool and treatment algorithm is provided, now also including strategies for patients with associated cardiopulmonary conditions. Treatment of paediatric PH continues to be hindered by the lack of randomised controlled clinical trials. The challenging management of children failing targeted PAH therapy is discussed, including balloon atrial septostomy, lung transplantation and pulmonary-to-systemic shunt (Potts). A novel strategy using a multimodal approach for the management of PAH associated with congenital heart diseases with borderline pulmonary vascular resistance is included. Advances in diagnosing neonatal PH, especially signs and interpretation of PH by echocardiography, are highlighted. A team approach to the rapidly changing physiology of neonatal PH is emphasised. Challenges in drug approval are discussed, particularly the challenges of designing accurate paediatric clinical trials with age-appropriate end-points and adequate enrolment.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: D. Ivy reports grants from the National Institutes of Health, GSK and Janssen, consultancy fees to the University of Colorado and support for attending meetings from Bayer, Merck and Janssen, and a leadership role with the Association of Pediatric Pulmonary Hypertension. E.B. Rosenzweig reports grants from National Institutes of Health, Bayer, Janssen, Insmed and SonVie, and is Director, PPHNet and Board Member, Team Phenomenal Hope. S.H. Abman reports consultancy fees from Chiasi and Oak Hills Bio, and leadership roles with BPD Collaborative and Pediatric Pulmonary Hypertension Network. M. Beghetti reports consultancy fees from Actelion/Janssen, MSD, Merck, Gossamer, GSK and Orpha, payment or honoraria for lectures, presentations, manuscript writing or educational events and support for attending meetings from Actelion/Janssen and MSD, and participation on a data safety monitoring board or advisory board with GSK, Actelion/Janssen, Gossamer, Altavant and MSD. D. Bonnet reports consultancy fees from Janssen, MSD and Novartis, and participation on a data safety monitoring board or advisory board with Lupin. J.M. Douwes has no potential conflicts of interest to disclose. A. Manes reports grants from Janssen/Actelion and Merck, payment or honoraria for lectures, presentations, manuscript writing or educational events from Janssen/Actelion, support for attending meetings from Dompè, and participation on a data safety monitoring board or advisory board with AOP Health Italy. R.M.F. Berger reports grants from Johnson & Johnson, consultancy fees from Johnson & Johnson, GSK and Ferrer, payment for educational events from Johnson & Johnson, Ferrer, AOP, MSD, Heart Medical, Occlutech Salveo, Bayer and Gossamerbio, participation on a data safety monitoring board or advisory board with MSD, and leadership roles with TOPP-registry, PPHNet and the ESC/ERS 2022 guidelines for diagnosis and treatment of pulmonary hypertension task force.
Figures
Comment in
-
The Seventh World Symposium on Pulmonary Hypertension: our journey to Barcelona.Eur Respir J. 2024 Oct 31;64(4):2401222. doi: 10.1183/13993003.01222-2024. Print 2024 Oct. Eur Respir J. 2024. PMID: 39209470 Free PMC article.
-
Reply to: Treat-and-repair: a simple but powerful term for a complex multimodal approach in patients with pulmonary arterial hypertension associated with congenital heart disease.Eur Respir J. 2025 Jan 2;65(1):2402127. doi: 10.1183/13993003.02127-2024. Print 2025 Jan. Eur Respir J. 2025. PMID: 39746763 No abstract available.
-
Treat-and-repair: a simple but powerful term for a complex multimodal approach in patients with pulmonary arterial hypertension associated with congenital heart disease.Eur Respir J. 2025 Jan 2;65(1):2402022. doi: 10.1183/13993003.02022-2024. Print 2025 Jan. Eur Respir J. 2025. PMID: 39746769 No abstract available.
References
-
- Beghetti M, Schulze-Neick I, Berger RM, et al. Haemodynamic characterisation and heart catheterisation complications in children with pulmonary hypertension: insights from the Global TOPP Registry (tracking outcomes and practice in paediatric pulmonary hypertension). Int J Cardiol 2016; 203: 325–330. doi: 10.1016/j.ijcard.2015.10.087 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical