

Adults with FPIES may face delayed diagnoses
- PMID: 39211327
- PMCID: PMC11359740
- DOI: 10.1016/j.jacig.2024.100304
Adults with FPIES may face delayed diagnoses
Abstract
Background: Food protein-induced enterocolitis (FPIES) is a non-IgE-mediated food allergy that is becoming increasingly recognized in adults. The time between age at symptom onset (ASO) and age at diagnosis (AD and factors affecting this gap have not been fully studied.
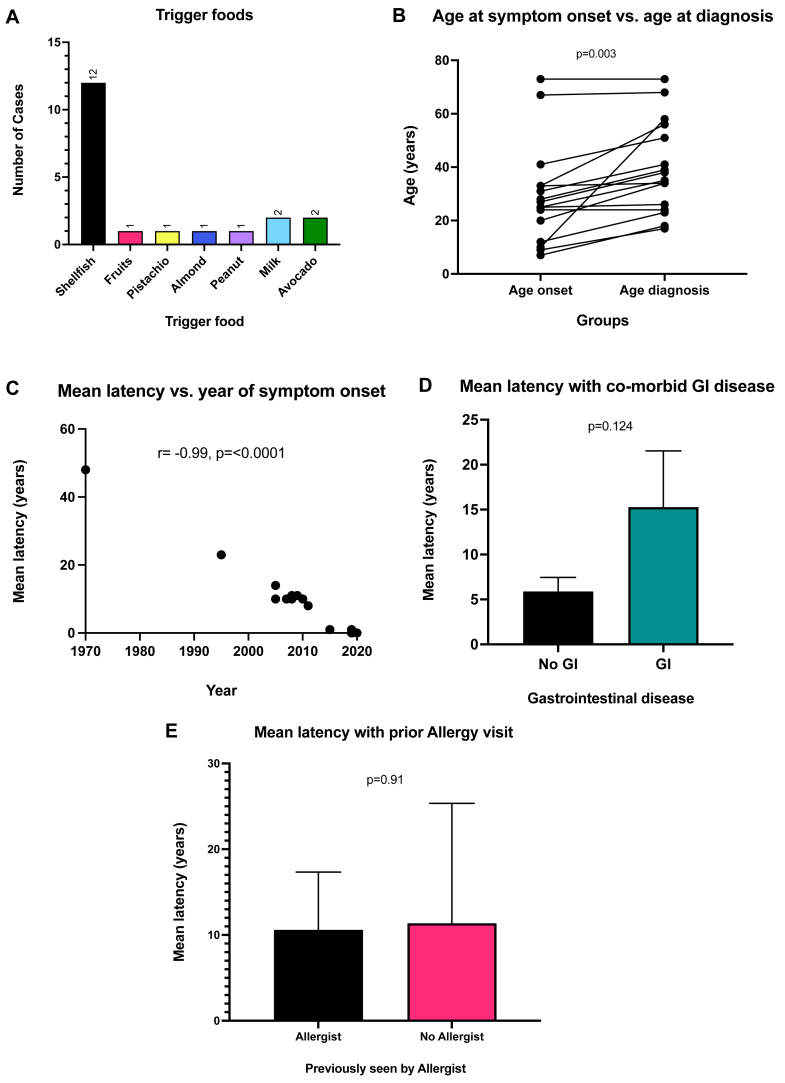
Objective: We sought to investigate the latency between ASO and AD in adults with FPIES. We also sought to evaluate whether those patients with symptom onset in earlier years and those with comorbid gastrointestinal (GI) disease had greater mean latency.
Methods: We conducted a retrospective chart review for patients with FPIES who were seen in the University of Michigan Allergy and Immunology clinic from 2015 to 2022. Patients aged 18 years and older and diagnosed with FPIES by an allergist were included (N = 19). The data collected included characteristics of the patients' prior FPIES reactions and medical history.
Results: The median age of onset of FPIES symptoms was 26 years, and the median AD was 35 years. The median difference between ASO and AD was 10 years; this difference was statistically significant according to a paired t test (P = .003). There was a negative correlation of -0.99 between year of symptom onset and latency between ASO and AD (P < .0001). Those patients with previously diagnosed GI conditions had a higher mean latency between ASO and AD than those without GI conditions did (P = .124).
Conclusions: We noted a gap between ASO and AD in adults with FPIES. This gap may be due to underrecognition of adult FPIES in the past given the negative correlation with mean latency between ASO and AD. Furthermore, comorbid GI illnesses may be masking FPIES symptoms in adults, thus delaying diagnosis.
Keywords: FPIES; Food protein–induced enterocolitis syndrome; adult FPIES; food allergy; oral food challenge.
© 2024 The Author(s).
Conflict of interest statement
This work did not receive or require direct funding. Related work was supported by the 10.13039/100007270University of Michigan via the Ronald Koenig, MD, PhD, 10.13039/100017094Department of Internal Medicine Early Career Endowment (to C.S.), the 10.13039/100001130Gerber Foundation (award 9026 [to C.S.]); and the 10.13039/100000060National Institute of Allergy and Infectious Diseases of the 10.13039/100000002National Institutes of Health (award K23AI162661 [to C.S.]). Disclosure of potential conflict of interest: The authors declare that they have no relevant conflicts of interest.
Figures
References
-
- Fernandes B.N., Boyle R.J., Gore C., Simpson A., Custovic A. Food protein–induced enterocolitis syndrome can occur in adults. J Allergy Clin Immunol. 2012;130:1199–1200. - PubMed
-
- Crespo J., Pérez-Pallise M.E., Skrabski F., Zambrano G., Rojas-Pérez-Ezquerra P., Noguerado-Mellado B., et al. The natural course of adult-onset food protein-induced enterocolitis syndrome. J Allergy Clin Immunol Pract. 2022;10:2986–2992. - PubMed
-
- González-Delgado P., Muriel J., Jiménez T., Cameo J.I., Palazón-Bru A., Fernández J. Food protein–induced enterocolitis syndrome in adulthood: clinical characteristics, prognosis, and risk factors. J Allergy Clin Immunol Pract. 2022;10:2397–2403. - PubMed
-
- Nowak-Węgrzyn A., Chehade M., Groetch M.E., Spergel J.M., Wood R.A., Allen K., et al. International consensus guidelines for the diagnosis and management of food protein–induced enterocolitis syndrome: executive summary—workgroup report of the Adverse Reactions to Foods Committee, American Academy of Allergy. Asthma & Immunology. J Allergy Clin Immunol. 2017;139:1111–1126.e4. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
