

Cardiovascular outcomes with semaglutide by severity of chronic kidney disease in type 2 diabetes: the FLOW trial
- PMID: 39211948
- PMCID: PMC11931213
- DOI: 10.1093/eurheartj/ehae613
Cardiovascular outcomes with semaglutide by severity of chronic kidney disease in type 2 diabetes: the FLOW trial
Abstract
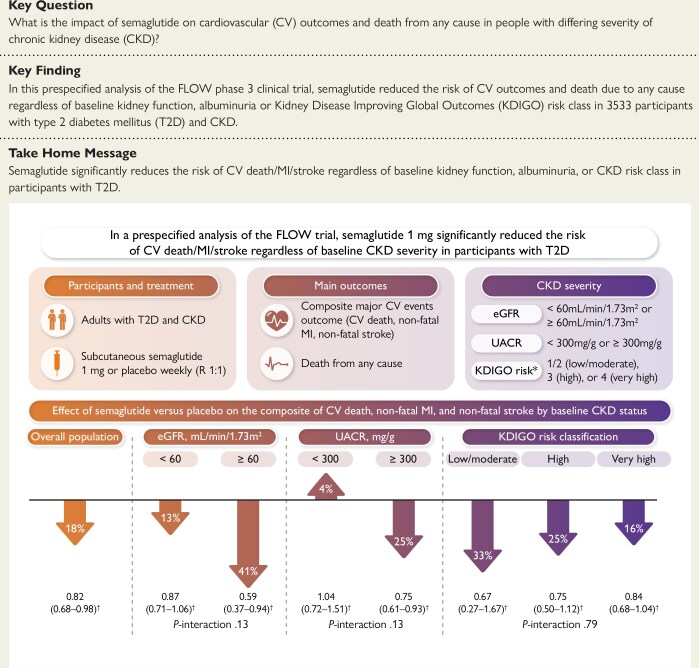
Background and aims: In the FLOW trial, semaglutide reduced the risks of kidney and cardiovascular (CV) outcomes and death in participants with type 2 diabetes and chronic kidney disease (CKD). These prespecified analyses assessed the effects of semaglutide on CV outcomes and death by CKD severity.
Methods: Participants were randomized to subcutaneous semaglutide 1 mg or placebo weekly. The main outcome was a composite of CV death, non-fatal myocardial infarction (MI), or non-fatal stroke (CV death/MI/stroke) as well as death due to any cause by baseline CKD severity. CKD was categorized by estimated glomerular filtration rate < or ≥60 mL/min/1.73 m2, urine albumin-to-creatinine ratio < or ≥300 mg/g, or Kidney Disease Improving Global Outcomes (KDIGO) risk classification.
Results: Three thousand, five hundred and thirty-three participants were randomized with a median follow-up of 3.4 years. Low/moderate KDIGO risk was present in 242 (6.8%), while 878 (24.9%) had high and 2412 (68.3%) had very high KDIGO risk. Semaglutide reduced CV death/MI/stroke by 18% [hazard ratio (HR) 0.82 (95% confidence interval 0.68-0.98); P = .03], with consistency across estimated glomerular filtration rate categories, urine albumin-to-creatinine ratio levels, and KDIGO risk classification (all P-interaction > .13). Death due to any cause was reduced by 20% [HR 0.80 (0.67-0.95); P = .01], with consistency across estimated glomerular filtration rate categories and KDIGO risk class (P-interaction .21 and .23, respectively). The P-interaction treatment effect for death due to any cause by urine albumin-to-creatinine ratio was .01 [<300 mg/g HR 1.17 (0.83-1.65); ≥300 mg/g HR 0.70 (0.57-0.85)].
Conclusions: Semaglutide significantly reduced the risk of CV death/MI/stroke regardless of baseline CKD severity in participants with type 2 diabetes.
Keywords: Cardiovascular outcomes; Chronic kidney disease; Semaglutide; Type 2 diabetes.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures





References
-
- Chronic Kidney Disease Prognosis Consortium; Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010;375:2073–81. 10.1016/S0140-6736(10)60674-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
