

Systemic inflammation and health outcomes in patients receiving treatment for atherosclerotic cardiovascular disease
- PMID: 39211962
- PMCID: PMC11578643
- DOI: 10.1093/eurheartj/ehae557
Systemic inflammation and health outcomes in patients receiving treatment for atherosclerotic cardiovascular disease
Abstract
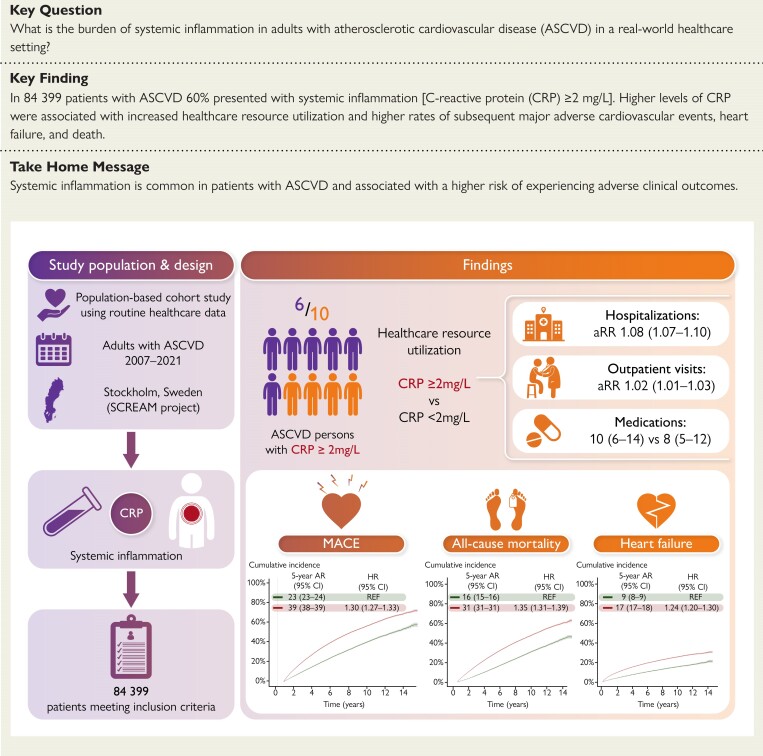
Background and aims: The burden and outcomes of inflammation in patients with atherosclerotic cardiovascular disease (ASCVD) are not well defined beyond the controlled settings of trials and research cohorts.
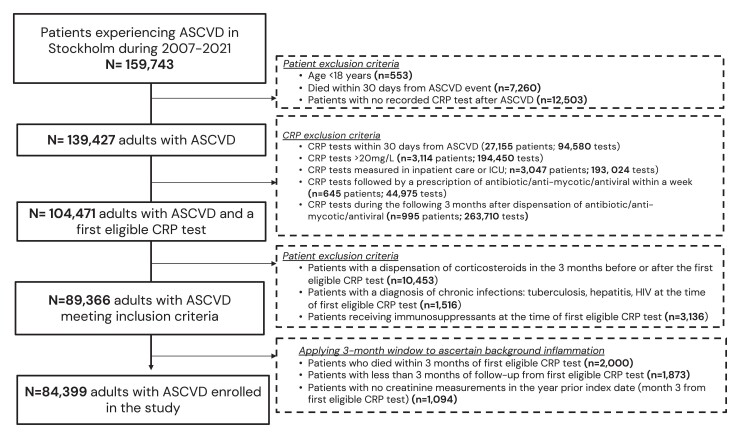
Methods: This was an observational study of ASCVD adults undergoing C-reactive protein testing in Stockholm's healthcare (2007-21). After excluding C-reactive protein tests associated with acute illness or medications/conditions that bias C-reactive protein interpretation, systemic inflammation was evaluated over a 3-month ascertainment window. Determinants of C-reactive protein ≥ 2 mg/L were explored with logistic regression. C-reactive protein categories were compared via negative-binomial/Cox regression for subsequent healthcare resource utilization and occurrence of major adverse cardiovascular events, heart failure hospitalization, and death.
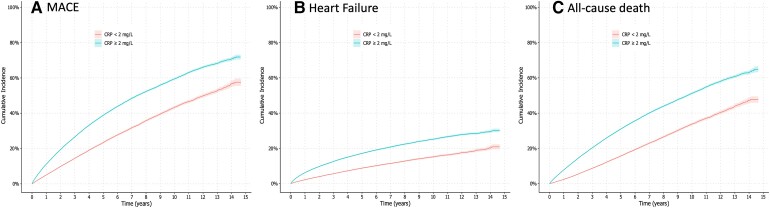
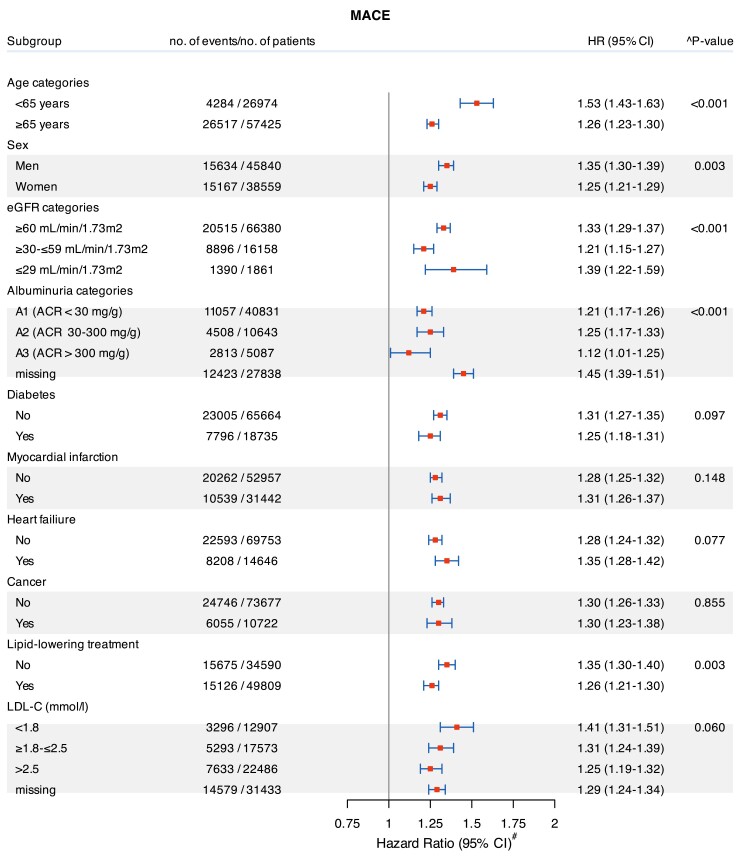
Results: A total of 84 399 ASCVD adults were included (46% female, mean age 71 years, 59% with C-reactive protein ≥ 2 mg/L). Female sex, older age, lower kidney function, albuminuria, diabetes, hypertension, and recent anaemia were associated with higher odds of C-reactive protein ≥ 2 mg/L. The use of renin-angiotensin system inhibitors, antiplatelets, and lipid-lowering therapy was associated with lower odds. Over a median of 6.4 years, compared with C-reactive protein < 2 mg/L, patients with C-reactive protein ≥ 2 mg/L had higher rates of hospitalizations, days spent in hospital, outpatient consultations, and dispensed medications (P < .05 for all). They also had a higher rate of major adverse cardiovascular events [hazard ratio (HR) 1.30; 95% confidence interval (CI) 1.27-1.33], heart failure (HR 1.24; 95% CI 1.20-1.30), and death (HR 1.35; 95% CI 1.31-1.39). Results were consistent across subgroups and granular C-reactive protein categories and robust to the exclusion of extreme C-reactive protein values or early events.
Conclusions: Three in five adults with ASCVD have systemic inflammation, which is associated with excess healthcare resource utilization and increased rates of cardiovascular events and death.
Keywords: Biomarker; CRP; Cardiovascular disease; Inflammation; Prediction; Prognosis; SCREAM.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
