

Prehospital Pulse-Dose Glucocorticoid in ST-Segment Elevation Myocardial Infarction: The PULSE-MI Randomized Clinical Trial
- PMID: 39211964
- PMCID: PMC11365011
- DOI: 10.1001/jamacardio.2024.2298
Prehospital Pulse-Dose Glucocorticoid in ST-Segment Elevation Myocardial Infarction: The PULSE-MI Randomized Clinical Trial
Abstract
Importance: In patients with ST-segment elevation myocardial infarction (STEMI), acute inflammation is related to the extent of myocardial damage and may increase infarct size. Thus, administration of pulse-dose glucocorticoid in the very early phase of infarction may reduce infarct size.
Objective: To determine the cardioprotective effect of prehospital pulse-dose glucocorticoid in patients with STEMI.
Design, setting, and participants: This was a 1:1 investigator-initiated, blinded, placebo-controlled, randomized clinical trial conducted between November 14, 2022, and October 17, 2023, with last follow-up on January 17, 2024. Patients 18 years and older with less than 12 hours of acute chest pain and STEMI were included in the prehospital setting throughout the Region Zealand and Capital Region of Denmark and transferred to Rigshospitalet, Denmark.
Intervention: Patients were randomly allocated to intravenous glucocorticoid (methylprednisolone, 250 mg) or placebo in the prehospital setting.
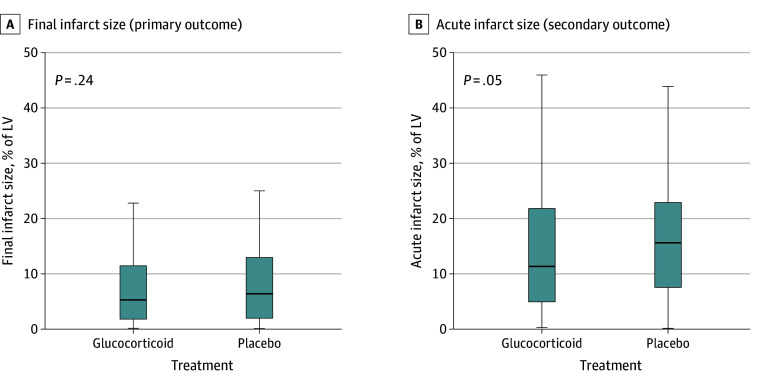
Main outcomes and measures: The primary outcome was final infarct size on cardiac magnetic resonance (CMR) at 3 months. The power calculation was based on an anticipated final infarct size of 13%. Secondary outcomes included CMR outcomes on acute scan and at 3 months, peak of cardiac biomarkers, clinical end points at 3 months, and adverse events.
Results: Of 530 included patients (median [IQR] age, 65 [56-75] years; 418 male [78.9%]) with STEMI, 401 (76%) were assessed for the primary outcome, with 198 patients treated with glucocorticoid and 203 with placebo. Median final infarct size was similar in the treatment groups (glucocorticoid, 5%; IQR, 2%-11% vs placebo, 6%; IQR, 2%-13%; P = .24). Compared with placebo, the glucocorticoid group had smaller acute infarct size (odds ratio, 0.78; 95% CI, 0.61-1.00), less microvascular obstruction (relative risk ratio, 0.83; 95% CI, 0.71-0.99), and greater acute left ventricular ejection fraction (mean difference, 4.44%; 95% CI, 2.01%-6.87%). Other secondary outcomes were similar in both groups.
Conclusions and relevance: In patients with STEMI, treatment with prehospital pulse-dose glucocorticoid did not reduce final infarct size after 3 months. However, the trial was likely underpowered as the final infarct size was smaller than anticipated. The glucocorticoid group had improved acute parameters compared with placebo.
Trial registration: ClinicalTrials.gov Identifier: NCT05462730.
Conflict of interest statement
Figures


References
-
- Desta L, Jernberg T, Löfman I, et al. Incidence, temporal trends, and prognostic impact of heart failure complicating acute myocardial infarction: the SWEDEHEART registry (Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies), a study of 199 851 patients admitted with index acute myocardial infarctions, 1996 to 2008. JACC Heart Fail. 2015;3(3):234-242. doi: 10.1016/j.jchf.2014.10.007 - DOI - PubMed
-
- Lønborg J, Vejlstrup N, Kelbæk H, et al. Final infarct size measured by cardiovascular magnetic resonance in patients with ST elevation myocardial infarction predicts long-term clinical outcome: an observational study. Eur Heart J Cardiovasc Imaging. 2013;14(4):387-395. doi: 10.1093/ehjci/jes271 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
